New Information
We have important new information about the impact of racism on the preterm birth rates in our country.
We now know that African American mothers who feel stress about the impact of racism on their children are more than twice as likely to give birth prematurely.
We also now know that the negative impact of the stress actually increases as both education levels and income levels rise for African American mothers.
We also now know that for actual infant mortality outcomes, the level of infant mortality goes down for our white mothers based on having higher education levels, but the infant mortality rate actually goes up dramatically as the education levels rise for our African American mothers.
That amazing and unexpected very powerful link between higher education levels and increased numbers of both infant deaths and early births for African America mothers is extremely important new information that we need to understand if we want to reduce either of those negative outcomes in our country.
It is widely known and frequently discussed public knowledge that we have the highest preterm birth rates in the industrialized world, and it is also widely known that those preterm birth rates and infant mortality rates are higher for our African American mothers.
People who are critical of health care policy and health care delivery in the US, often point to our very high rates of both premature birth and infant mortality as proof points for the shortcomings of our system for both care and coverage.
What we have not discussed with any sense of confidence was what specific and explicit factors were triggering those negative outcomes for American mothers.
We have speculated about disparities in care delivery, prejudiced approaches to care, stress factors during pregnancy, and possible economic factors that possibly created those significantly differences in care outcomes.
We now have much better information on those topics — and we can now report with some levels of confidence that racism and related stress factors are actually extremely significant factors for both our prematurity rates and infant mortality rates.
New research from excellent teams at Duke University, The University of California at Berkeley, The New York Academy of Science, the University of Michigan, and several other highly competent settings have just given us important insights into those extremely negative performance levels for both preterm birth and mortality levels.
One of the least expected findings was that higher education levels and higher income levels actually increased both of those negative outcomes for our African American mothers.
Much Higher Infant Mortality Levels for PhD Mothers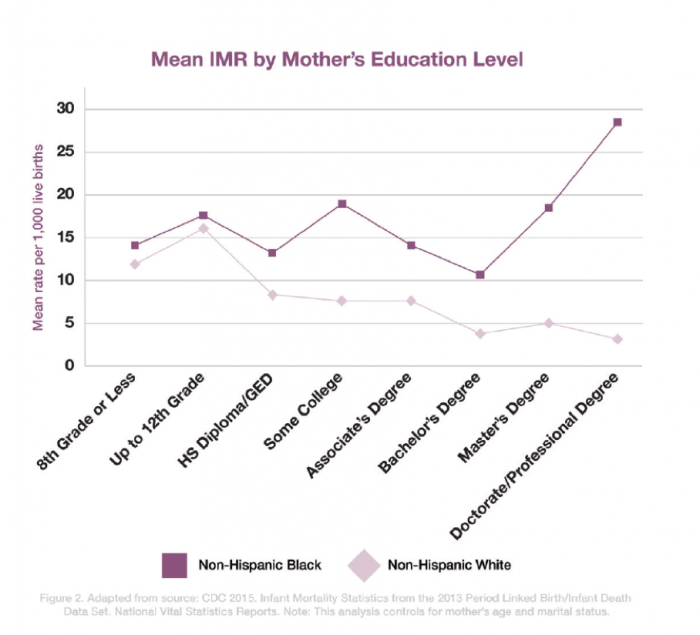
The chart directly above these words has information that deeply surprises most people who see it for the first time. The extreme contrast between White mothers with PhDs and African American Mothers with PhDs seems to be almost unbelievable. But both charts are real — and we now need to build those learnings into our thinking about care in America.
We owe the University of California at Berkeley a deep debt for discovering that extremely important link between preterm birth rates and racial stress perceptions by pregnant women and we owe Duke University an equally deep debt for discovering that second set of outcomes between education levels and those negative outcomes for African American mothers.
We owe The Center for American Progress a debt for writing an earlier piece that directly linked racism to those issues. We also now owe the New York Academy of Science a deep debt for looking at those issues and findings and publishing information in late 2019 about the allostatic load data and impact on African American mothers that gives us a key biological connection that further explains those amazingly important and previously unexpected and unknown outcomes and linkages for those mothers.
The Berkeley study, the Duke study, and the Center for America Progress piece all showed that the prematurity rate increased for African Americans and decreased for White Americans based on having higher education levels for the mothers and the New York Academy piece on “The Superwoman Schema” helped explain why from a scientific perspective why that was true.
This is very important new information for us as a country. We have significant failings in each of those areas, and we are more likely to make significant improvements in those areas if we better understand the factors involved.
People debating and discussing health care reform in America often point to the fact that we spend more money on health care than any other nation by a wide margin and yet we have some of the highest and worst premature birth rates in the world as a nation — and the people who make that point often reinforce their argument by pointing out that those birth related numbers are actually getting worse.
More than 130 other countries have lower preterm birth rates than we do. The fact that large numbers of our children are being born prematurely is one of the reasons our infant mortality rates are among the worst levels in the world and that fact also adds to the significantly higher health care expenses that we have as a country because the care for premature infants can easily total hundreds of thousands of dollars for each child.
We currently have the highest number of babies who die the day they are born of any country in the industrialized world.
By contrast, the preterm birth rates in the most successful countries last year for that birth outcome were 5.5 percent of births in Ireland, 5.6 percent of births in Finland, and 6 percent of all births in Greece.
Success Levels
We know from the success levels of those countries that significantly lower premature birth rates are both possible and affordable.
That is not a new situation for us to be in. We have known for years that we have some of the worst preterm birth rates in the world — and we also have known that our disproportionately high levels of premature births are not distributed equally across all groups of mothers in our country.
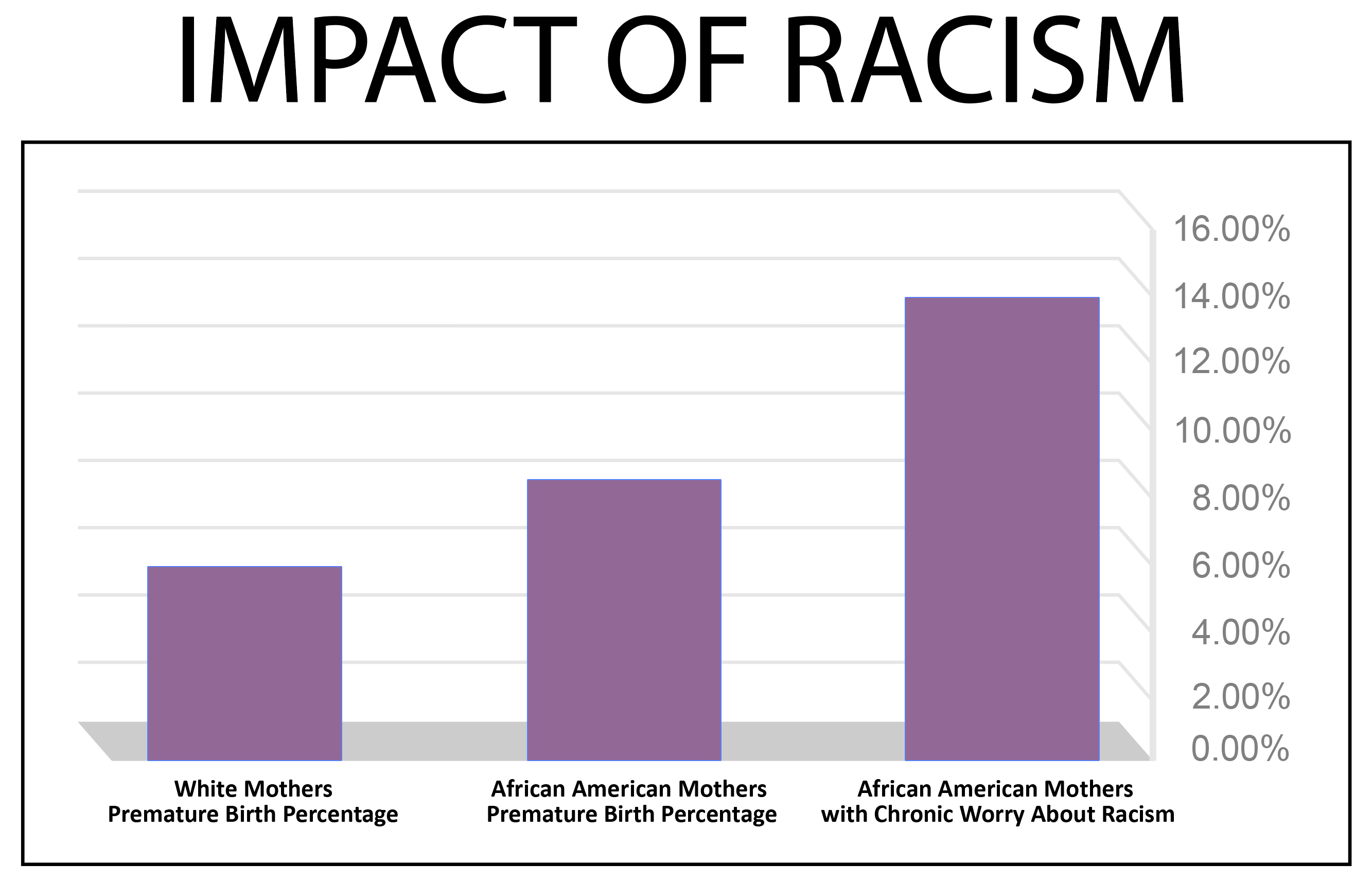
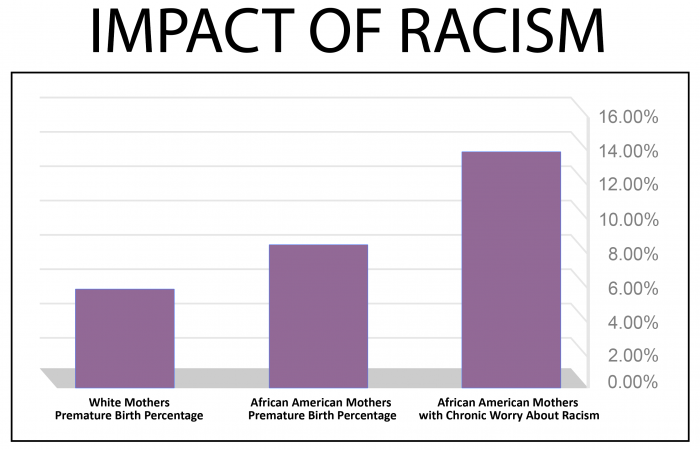
The prematurity rate is now slightly below 9 percent for our births for our white mothers — a number that was far from the best level in the world but is near the top of the range.
The prematurity rate is, however, at the very top of the range on the negative side for our African American mothers.
Last year, nearly 14 percent of births to African American mothers were premature.
Multiple theories have been proposed about those issues and a number of studies have been done — but there has not been a good set of answers until now that have explored the problem or explained those differences in results and in patterns between groups.
Several earlier studies have shown that high school graduates and college educated white and Asian American and Hispanic mothers had significantly lower premature birth rates than high school drop outs from each of those groups.
But for our African American mothers, those earlier studies did show and note that the premature birth rate actually increased with higher education levels and with higher income levels for African American mothers. The Center for American Progress Racism piece reported that data — but only partially quantified the situation and did not explain it.
Duke did an extremely important job of quantification on multiple aspect of the prematurity problem — and their education level links were groundbreaking discoveries/.
Duke looked with great insight into a number of factors that were driving infant mortality rates in the US, and concluded that race related issues were very important to those outcomes. Their work added a significant layer of learning by drilling down into actual education levels for the mothers.
Duke University just did a very powerful analysis of education impact by group on preterm birth that went to a higher level of detail and looked very specifically at the exact levels of education for each of the mothers.
They added basic education degrees for the mothers to their analysis of mortality rates for the children and they linked the exact education levels of the mothers from both groups of mothers to the mortality rates for their children.
That turned out to be extremely useful and somewhat startling information
When the researchers at Duke looked at mortality rates and education levels of mothers, they found that the mortality rate for white mothers with an eighth grade or lower education level was 12 births per thousand births. As expected from other studies, they reported that the mortality number dropped to 5 of the births when the white mothers had a master’s degree.
That number dropped even further to only three deaths per thousand when the white mothers had a PhD or equivalent education level.
That means that the Duke data for white mothers showed clearly that higher levels of education actually had a significant and positive reduction impact on the infant mortality rates for those mothers, and the white mothers with PhDs had some of the very lowest infant mortality rates in the world — far better than the results from any other country that measures those results.
However — their research then confirmed the other studies that had also found the exact opposite impact on the rate of preterm birth for African American Mothers, and the researchers at Duke discovered that African American mothers with PhDs actually have among very highest mortality rates of any mothers in the world who are not in an active war zone.
We now have good data showing us that higher education levels actually increased the rate of preterm birth percentages for the African American mothers in both of those studies — and higher education level for that set of African American mothers studied by Duke also increased the mortality rate for their births.
We need to understand those numbers as a country and as a care system.
The Duke researchers reported that the African American mothers with an eighth-grade education had a 15 babies per thousand mortality rate — a number that looks very much like the current national average for African American mothers.
However, they discovered that when the African American mothers had a master’s degree, the mortality levels actually increased to 19 of the births.
That outcome became even worse as education levels rose
The Duke team discovered and reported that when the African American mothers had a PhD or equivalent degree, that infant mortality number for those mothers jumped to 28 of the births.
That number is almost double the rate for the African American mothers who dropped out of school and it is actually ten times higher than the rate for White mothers in America with a PhD.
So the impact of having a graduate degree or a PhD had a significantly different impact for preterm birth rates and the infant mortality rates for each set of mothers studied by Duke.
That is very important information for us to have and it isn’t information that people in our care delivery world or public health infrastructure have been building into their thought processes for either premature birth or education issues before now.
They concluded that various kinds of stress related to racism probably caused those very different results and their team speculated very logically and insightfully that the personal stress levels relative to racism might can be higher when African American women have higher degrees.
The Duke study stated that the damage was done by “increased experiences of discrimination and stress as Black mothers attain higher levels of education.”
The Duke team also reported that “Reports of encounters with racial discrimination are higher for blacks that live in predominantly white middle class neighborhoods.”
California Study of Stress During Pregnancy Proves a Direct Racism Link
That thinking about those particular stress points has now been entirely confirmed and partially quantified by the other two studies cited above
That impact was explained biologically by the New York Academy of Science thought piece on that same issue and that direct impact relative to racial stress issues has now been quantified in very direct ways by the new Berkeley research.
The new Berkeley study was focused on specific causes of stress during pregnancy that might trigger premature birth. The Berkeley and State of California research team actually looked in very systematic and insightful and effective ways at multiple causes of stress during pregnancy to see what impact each type of stress might have on the prematurity levels for the mothers.
The California research looked specifically at multiple levels and types of stress during pregnancy for the California mothers in their study.
That California study found the same inverse differences in the rate of preterm births for African American women and white women relative to their personal education levels and income that the Duke data and the Center for American Progress had uncovered relative to infant mortality.
The new research also showed that the African American mothers in California with higher education levels were more likely to give birth prematurely than women with lower education levels, and it also echoed the Duke data and showed that white mothers in California with higher education levels were less likely to give birth prematurely than white women with lower levels of education.
The researchers, for the first time ever, looking directly at a dozen specific and explicit stress factors that can happen for mothers during a pregnancy.
The researchers looked at the impact of specific stress factors during the pregnancy for each set of women for the first time ever in a research study on pre-term birth.
They looked at issues like homelessness during pregnancy, domestic abuse, drug use, smoking, food shortages, and concern about the negative impact of racism on your child.
The attached research that investigated those issues and reported those findings was presented to The California First Five Commission for Children and Families at their July, 2018 meeting.
The First Five Commission was created and funded by the voters of California as an initiative to help children and families in that state, and looked at the data because the scope of the Commission concern extends from Zero to Five years old and the premature birth rate numbers were obviously a problem for the state.
The California Commission reviewed the new research data about the impact of stress during pregnancy as a factor that can influence success levels for children in the first five years of life, and concluded that the linkages between racism and pre-term birth were very real and important to address.
The researchers looked at more than 10,000 births in California as their core research subject matter.
California studies ten thousand births every year as part of their public health agenda as a state. They had never before looked at specific stress factors as a key topic of the research.
The researchers very intentionally and carefully identified multiple key stress related issues and factors relative to each of the mothers who gave birth during that time frame.
Their goal was to look at multiple stress points during each pregnancy in an attempt to discern or determine what stress related issues and factors might currently have the biggest negative impact on the premature birth rates for California mothers.
Medical science and medical practitioners have known for a number of years that higher stress levels during pregnancy increase prematurity rates — but what researchers did not know before this research was done was exactly which stress factors were most relevant to higher levels of premature births.
The California research team did very important, innovative, useful and insightful work on that issue.
The researchers identified a dozen key and explicit stress factors for the mothers.
They gathered baseline and foundational data about the age, the income and the education levels of the mothers.
Job Loss, Violence, Separation, Health Comorbidities, and Racial Stress Were Included
The research team carefully identified very specific and explicit stress factors during pregnancy for each mother — like loss of jobs, income stress, food shortages, multiple health conditions, domestic partner violence during pregnancy, divorce, separation during the pregnancy, binge drinking, smoking levels and whether the mothers worried about the impact of racism on them or their family.
It looked at each of those stress factors alone and looked at them in all possible combinations to determine their relative impact.
The study of all of those births produced by that research is attached.
That study has extremely useful information about the extent of each and all of those stress factors on the mothers. It gives us great and useful baseline data on a number of new maternal stress factors for future research as well as giving us highly useful information about the relative impact of each of those stress issues on premature births now.
The research team looked at all of the premature births and did statistical analysis to see which stress factors during pregnancy, either alone or in combination with other specific factors, actually increased the likelihood of premature birth for the California mothers.
Their numbers and the linkages they discovered to the stress factors tell a powerful story that very directly quantifies and reinforces earlier work done by The Center for American progress on those issues.
In looking at the overall rate of preterm birth, the Berkeley study found that 5.8 percent of the white mothers studied in that year gave birth prematurely. They discovered that 9.2 percent of African American mothers in California gave birth prematurely.
They then looked to see which of those dozen explicit risk factors that they identified had the biggest impact on the premature birth rate for African American mothers.
They believed before doing the research that the racism issue would have an impact on the rate of premature births, but they did not expect the relative force and the disproportionate and major impact of that particular stress factor on the rate of premature birth for the African American mothers in California.
Racism won.
Racism very clearly had the biggest impact on the rate of premature birth for that set of mothers in the California study, and the impact of racism stress was significantly higher than all of the other stress factors combined.
The African American mothers who reported worry about the impact of racism were far more likely to give birth prematurely.
Racism Stress Significantly Increased Preterm Births
Slightly more than a third — 39 percent — of the African American mothers reported that concern about racism for them or their family in the survey.
Those mothers had very different birth results.
The mothers who expressed that concern about the impact of racism were more than twice as likely to have a premature birth as white mothers in California.
For those African American mothers who reported that worry, 12.5 percent gave birth prematurely.
As the important studies done by the Duke researchers and by the Center For American Progress study had also noted, the Berkeley researchers also found increased premature birth rates for the mothers with that worry were highest for the African American California mothers with the highest education levels and the highest income levels.
We now know from that study that the African American mothers with higher education levels and higher income were significantly more likely to worry about racism for themselves and their family — and we can conclude that the increased level of stress created did exactly the kind of biological damage that researchers have known for years results from stress experienced by a mother during pregnancy.
The New York Academy of Science paper on that issue now explains and describes the allostatic load process that is biologically accountable for those results. Their timely and insightful paper — “Racial Discrimination, the Superwoman Schema, and Allostatic Load Stress Coping Model Among African American Women” — helps anyone wondering how that linkage could happen understand what is actually happening for each of those mothers.
Thanks to their thinking, we now have a better understanding of the science involved and those outcomes make better biological and psychological sense.
So we now know from very good research that worry by a mother about the future impact of racism on your child is actually the very best predictor we have now of preterm birth that we have in America.
That major damaging impact that results from the worry about racism on women giving birth is important for us all to know. It explains why that set of mothers has had higher rates of premature births for decades, in spite of the fact that the health care system, itself, had not seemed to be significantly different during the pregnancy for those higher income mothers.
That new set of insights might also explain in part why some doctors have failed some of those high-risk mothers when the mothers have reported problems during pregnancy because the doctors probably thought of them as being low risk patients and the doctors sometimes did not respond quickly when negative events started to happen for those pregnancies and deliveries.
We need all relevant doctors to know this full set of information — and we particularly need doctors who help African American mothers from all groups to understand more clearly who their highest risk patients actually are in America today.
We also should very intentionally and effectively reach out directly to those high-risk mothers in a number of ways.
That very powerful set of data should now cause us to do some targeted and effective support for those mothers, that might help to reduce pregnancy related stress in some way for those mothers during that period of time.
We need targeted outreach to all of the high-risk mothers that begins by sharing this data and explaining its consequence to each mother and her care team. We now know the high impact of ACEs data on other health care issues, and we need to extend what we are learning there on interventions to help I coaching and supporting this set of mothers.
We also need to recognize that this extremely important information only explains part of the problem of having too many premature births for our country.
Those extremely important numbers about that particular type of stress do not explain the entire situation and they do not account for the entire difference between the premature birth rates in either California or the rest of the country. We now know that, overall, 12.5 percent of the African American mothers in California who reported having that worry about the impact of racism had a premature birth.
However, we also know that compares to a 7.2 percent premature birth rate for the African American mothers in California who did not report that concern for the survey.
That 12.5 percent premature birth rate and the 7.2 percent numbers both compare to a 5.8 percent premature birth rate for the white mothers in the study. So we clearly have additional opportunities for care improvement for all of those mothers to bring down the preterm birth rate even further.
At a core level, however, it is very important for us all to understand that those mothers with that Racism worry were more than twice as likely to give birth prematurely, and we also need to know from the Duke study that the infant mortality rate can more than triple for African American mothers with higher levels of education and income.
We need far more research to drill down into those findings at multiple levels. That information about those birth outcomes is just the tip of an iceberg of relationships and realities that we need to understand. More research, analysis and expert thinking needs to be done to understand that situation more completely.
But that particular number tied to that concern in this study is extremely important information for us to have because it shows that racism has a direct and powerful impact on the premature birth rates in this country, and it is clear that we definitely need to use that information about that impact in some useful ways simply because we now know it.
Important knowledge can create its own obligation level and its own ethical requirement for use by people who learn it when the information is truly important.
We need to improve our knowledge about the issues of racism and pregnancy damage, and some important thinking and research on those topics is being done.
Danyelle Solomon wrote the very powerful piece for the Center for American Progress on racism and births that was noted above that very clearly described many of those same issues and she also reported that strange unexpected relationship between higher income levels and higher rates of preterm birth for African American mothers.
Solomon helped tee this set of issues up for the country — and did not have that final link from the brand-new California Research that tied higher levels of premature births to having that concern about racism in a measurable way — but she did predict that it would exist — and she was correct in her assessment and prediction.
The University of Michigan just released a major study that also looked at birth related problems for African American women that goes beyond preterm birth rates into other related health issues and deals very directly with some important disparities in the delivery of care.
All of those studies are important — and the information about the stress damage caused by the Racism concerns are very high on the list of things we need to understand and address as a country.
Now that we understand this information about the impact of those concerns, we have an ethical, logistical, moral, and functional obligation to use that information in beneficial ways.
Knowledge is power and knowledge about relevant information directly triggers accountability. We need people who are working on issues of premature birth to understand this information and these processes and to be able to factor it into their thinking about this entire set of issues and processes.
We Need Every Pregnant African American Woman with a PhD to Understand Those Findings Now
We particularly need to use and share this information about the impact of those particular concerns immediately with every African American woman with a master’s degree or a PhD or a law degree or any equivalent education level who is expecting a child or who is planning to have a child.
We need every obstetrician who is taking care of African American mothers with higher levels of education to recognize that they have a high-risk patient and they should take every medical precaution to help bring that pregnancy to full term.
We need targeted and better-informed physicians and care teams, and we need families and communities to offer emotional and functional support to those high-risk mothers.
If nothing else, we need to have people who care for each patient to give a respectful and loving hug equivalent and a warm and clear level of support to each pregnant African American woman to help reduce the new mother’s current levels of stress at this exact highly relevant point in time for each mother.
We very obviously need every African American woman in this country with a master’s degree or PhD who plans to have a child to know that information about that impact and those outcomes immediately.
Sharing that information with every African American woman with a PhD or a master’s degree should be possible for us to do if we each take that obligation seriously because the Internet can reach everyone and we all need to be personally accountable to extend that information to every relevant person in every way that we can reach that set of women as soon as possible.
We can’t end racism or make it less threatening and damaging — but we can mitigate and work to reduce stress for individual people in direct and caring ways at important key points in time that can help increase the likelihood of a full-term birth for those mothers.
The next question that we need to deal with is — so what do we do with that entire set of information about the impact of racism on births once we know it?
We Need to Share that Information with the People who Are Most Damaged by that Stress
We need care givers and family members and friends, and community members all to be sympathetic and supportive and to do a wide range of things to help reduce the stress levels for African American expectant mothers with a particular immediate focus on the mothers who are most affected by this information.
We unfortunately are unable to end or eliminate racism. Racism is a problem for us as a country that we do clearly need to address at multiple levels, but we can’t solve those issues quickly enough to have a positive impact on children who are in the hospital being born at this very moment.
We are and have been a racist country at many levels. We have been improving relative to racism in very good ways in a number of important areas — and the very fact that there were enough African American mothers with master’s degrees and PhDs to be a statistically valid category, sample and measurable group in the Duke study tells us that we have made some progress in some areas. That number of African American mothers with graduate degrees would have been much smaller 20 years ago and it would have been statistically invisible or non-existent 50 years ago.
Progress has been made in some key areas related to racism, and we should celebrate and build on that progress.
But we also need to understand and accept the truth that we are far from resolving those issues of racism as a country at this point in time, and we should all recognize that the worry felt by those mothers about racism is entirely legitimate and accurate and prescient and appropriate and entirely valid at both functional and social levels at this point in time for each of those mothers because racism exists and because racism is doing damage to real people in our country today.
We Need to Take Steps to Reduce Racism and Inter Group Anger
We need to understand those issues that link to racism and inter group anger and division — and we need to recognize that we need to take steps now as a nation to remedy them, because if we don’t deal effectively now with those issues that divide us, we are at risk of going down the same ugly and destructive paths that are happening today in over 200 settings in the world today where people are killing each other based on Us/Them instincts and based on their inability in those settings to be aligned and at Peace with each other.
The InterGroup Understanding books and website education and thought pieces about instinctive inter group behaviors explain why we have those racist components to both our history and to our current inter actions as a people, and why it is so dangerous to activate our Us/Them instincts and identify other people as Them in any setting.
To create a safe and internally aligned America — and to end some of those damaging inter tribal and inter group behaviors, emotions, and beliefs as an American people — we need to understand why we have those beliefs and we need to understand what we need.
The mothers who feel worry about the damage that racism might do to their family have very appropriate concerns. We have some people in our country today who have slipped into the mind sets of division and negative inter group behaviors — and that is a slippery and seductive and self-reinforcing slope once people actually go down it.
The internal conflicts we are having today in many communities and as a nation in some very visible ways will not disappear of their own accord. We need to do the right things and we need to do them well to succeed as a nation and as a people at multiple areas.
We have choices. We can have a wonderful and successful future as an aligned and mutually supportive nation, and we can leave our grandchildren a future where they are both successful and safe instead of being at war with one another.
Or, we can choose an ugly, dysfunctional and damaging future of division, anger, inter group conflict and inter group separation — and we can give our grandchildren a future where they will very likely need to be armed in their own homes because people from other groups will want to damage them or kill them because they are from a hated group of people and because our pathway as a nation to high levels of inter group diversity is irrevocable, inevitable and clearly destined to be our functional reality.
We should choose to have America be a wonderful, and supportive place where our grandchildren are safe, prosper, and thrive.
To achieve that goal, we need to make clear, intentional, and direct commitments to each other as an American people to help all of our groups thrive and prosper and do well.
We Need Children from Every Group to Get the Right Support in the First Months and Years
As part of that commitment that we make to each other, we need to give children from every group the right levels of brain strengthening and neuron linkages in the first months and years of life that will end and prevent the major disparities we have in our education and prison systems today.
There are a number of things we need to do as a country to give our grandchildren a future where we will not look just like a hundred other multi-group countries in the world who currently are at war with themselves.
The InterGroup books explain those conflicts in those other countries today as well. Syria, Sri Lanka, Fiji, Yemen, and a hundred other multi-tribal nations currently have people whose most negative inter group instincts are fully activated who are very intentionally and very deliberately doing damaging things to one another every day. We all have those sets of instincts — and we cannot allow them to be activated at those kinds of ugly and damaging levels here.
This particular study of the impact of racism on California births has an immediacy to it that should lead us to do things now for a number of mothers that will help reduce the number of preterm births in this country. We now know from the great research done at Duke that there are some mothers at highest risk — and we should each reach out now to all of those mothers to reduce their risk and to help them have healthy, happy full-term babies and births.
We need our best and brightest caregivers to work together to support all African American mothers relative to those issues.
A couple of organized care systems who saw that report that was made to the California First Five Commission for Children and Families two months ago about the impact of that racism stress factor are beginning to do work in those areas. We need to learn from their efforts and we need to share them with other caregivers and communities in the country.
We can make a difference. That difference needs to be made.
Please share this information with anyone who might be thinking or working with those mothers and those care sites where the premature birth rates are the highest in the world.
Also — please share both the Duke study and the California study with anyone who might be able to share it with any African American mothers who might somehow be in your world.
Now that we have this particular knowledge, we need to use it to change the future for a number of people in important ways that will enhance lives and give us all a better result.