
We have just achieved a total health care expense for our country of more than $4 trillion for last year, and that number will continue to climb at an unaffordable rate for the foreseeable future unless we do something relevant and useful about it.
We should do that.
We are doing almost nothing as a country to have a positive impact on that trajectory — and that is unfortunate, sad, inadequate, wrong and unnecessary because we actually do have one current purchasing tool that we know can both improve the quality and the effectiveness of care and reduce the costs of care for significant numbers of people at the same time and that tool is in place now doing some heavy lifting for people and processes and settings who deserve and need to be lifted.
Most people do not know that tool exists.
The overwhelming majority of people — including high percentages of our most relevant academics and a very high percentage of our health-related journalists and media people — do not understand today what that tool can do and they do not understand or appreciate both how it does what it does and why we can have confidence in its future success based on current performance and based on understanding layers of structural components that have been carefully, intentionally and competently built into the process over the past decade or so to allow that purchasing process and that care improvement success to succeed.
The Tool is Medicare Advantage
We have overwhelming proof at several levels that we get better, continuously improving and less expensive care for significant numbers of Medicare enrollees and patients through that tool.
Those achievements are a success for the specific purchasing process that is used to buy that care. That better care for millions of patients has happened because the business model of Medicare Advantage is to use a capitation cash flow to pay for the care — rather than buying the care for those members entirely by the piece. Capitation can be set up to both incent and enable better care.
The business model of capitation creates financial gains for care teams when care is more effective and more efficient rather than the purchasing model for care that we usually use for our Medicare patients of having the caregivers rewarded financially and given additional money when their care is inadequate, insufficient, ineffective, underperforms or fails.
That’s the badly flawed payment model and the cash flow reality that we get with the traditional Medicare fee-for-service payment model that we use to buy most care for both Medicare and that we use in almost all care settings for multiple other sets of patients and other care providers in America who are paid only fees for their care.
The results at the care delivery level could not be more different for the Medicare Advantage members than for the fee-for-service Medicare patients — with lower rates of hospitalizations and better care happening for Medicare Advantage patients at an overwhelmingly obvious level.
The costs and outcomes have been very different, but the frustrating reality is that those sets of care differences and those achievements by the Medicare Advantage plans have not been observed or understood by far too many people who should know that those successes exist as we are trying to figure out how to create both lower costs and better care for America.
Too many experts don’t understand what is happening with that care for both Medicare Advantage and fee-for-service Medicare.
Many people looking at health care issues don’t link the fact that the Medicare Advantage plans use 35 percent fewer emergency room visits and more than 40 percent lower inpatient hospital days for several sets of chronic care patients as actual and immediate proof both that the care is better when people don’t need to be hospitalized and that the care is much less expensive for us all when those sets of hospitalizations are not needed.
The $4 trillion we spend on care as a nation actually goes down by a bit as a total cost each time we reduce the length of stay or avoid a hospital admission because each reduction is a care expense that doesn’t happen and that isn’t in the total spend and that will not trigger a bill at any point in time.
The key point is that Medicare Advantage is delivering better care to those patients and doing it for less money and actually bringing down the total cost of care for the entire country by achieving those goals.
We have managed to fail fairly badly in explaining, sharing and linking those results with our most relevant health policy, academic, and health media settings that those results and those successes are far too often neither seen, understood, or appreciated today.
Medicare Advantage has relatively little public policy support today for most of those agendas — even though we have strong proof that it is actually doing that job by delivering better care and it is true that proof of that better care is fairly easy to see at multiple levels once you understand what it is and learn to recognize it as actual proof.
We should be able to earn that support for Medicare Advantage from many more of those people because the approach works so well.
We know that the people who are enrolled in our Medicare Advantage plans are half as likely to go blind, half as likely to have amputations, and less than half as likely to be hospitalized for multiple conditions when they are in the system and when they are using the basic and relatively obvious to see care resources of the plans.
That’s better care — and far too many health care economists and health care policy people don’t understand what it is and why it’s important to our future purchase of care to provide better care to our Medicare population and to do it for less money.
Look at the new and confirming data from multiple sources. Medicare Advantage patients in the groups with serious medical conditions had a 29 percent lower rate of avoidable hospitalizations, and a 41 percent lower level of avoidable acute care condition hospitalizations.
One of the key performance level successes for the Medicare Advantage plans is to have a 71 percent lower rate of diabetes related complications for our lowest income and our highest need dual eligible patients.
Those are very real and important differences in performance between the two approaches. The lives of real people are affected every day in very important and extremely relevant ways based on which Medicare funding track they have chosen to go down — and the people who have chosen Medicare Advantage instead of fee-for-service Medicare are now less than half as likely to have a limb amputated over the next couple of years because their Medicare Advantage plans are doing targeted things with patients to keep that from happening.
Special Needs Members Get Much Better Care
We have much better care for most of the patients who are getting more focused care and we now have extremely good care for many of the 4 million people enrolled in Medicare Advantage special needs plans who create direct and targeted support for each of those patients. People in policy settings do not understand how poor some of the Medicare fee-for-service care is — and the results of that bad care show up in that Shameful Metric care information and the truth is that those horrible care screw ups in that Diabetic Amputations “Shameful Metric” research piece are not happening for the Medicare Advantage patients because every patient has a link to actual organized care and to Medicare Advantage caregivers who are not allowing those care disasters to happen.
The blood sugar successes for the Medicare Advantage plan caregivers tracked by the Medicare Advantage five-star quality plan just improved slightly during Covid and they amputation levels are getting worse in patients who are not included in the care construct created by the plans.
Fee-for-service Medicare has created and sustains that Shameful Metric approach to care by not having any care coordination, no care data sharing, and no systematic approaches to care for those patients who are having amputations and going blind. The capitated Medicare Advantage plans do the exact opposite and it’s the right thing to do because people in the plans have much better lives and fewer lost limbs.
We need people who are thinking about health care policy issues to know that those massive and life changing care differences exist and we need everyone to understand the clear and basic reasons that those huge differences in care patterns and in care outcomes exist between fee-for-service Medicare and the Medicare Advantage plans.
That’s not rhetorical.
We have large scale proof and significant amounts of evidence on each of those points of difference.
The Medicare Advantage patients who are Dual Eligibles are the perfect example of performance in both directions, because we can see easily how bad care is for dual eligibles who have not joined Medicare Advantage plans.
The dual eligible are all of the people in this country who are eligible for both Medicare and Medicaid. They are the highest care needs and the lowest income subset of the patient population in each of their age groups. Medicare Advantage does extremely good work for those patients and standard fee-for-service Medicare underserves many of them so badly that it’s almost criminal behavior for the rest of us to allow that to continue to happen to those dual eligible people without doing something to help them.
It is extremely good for our country that we have enrolled 4 million of our lowest-income and our highest medical-need patients in the Medicare Advantage plans. The data from multiple sources and perspectives shows that their care has often been exceptional in a number of key areas and that lives are better for millions of people who are eligible for both Medicare and Medicaid because the Medicare Advantage plans have taken on those patients and delivered systematic, patient focused care to them on an individual patient specific basis.
The people who look at that reality in functional terms also know that people who understand those related basic care processes for patients can do important things to change the care trajectories for many of the 5 percent of our people who create 50 percent of our total costs if they can just get them into care settings and into care processes that cause and allow that much better care to happen.
The capitated Medicare Advantage plans put patient focused care approaches in place for those high opportunity patients, and those science-based process engineered approaches that are used by the plans actually do work to make care better and less expensive for those patients and that collective success actually gives us a chance to change the cost trajectories for care if we do it for enough people.
That isn’t a hypothetical or theoretical or even an ideologized and politicized basic suggestion for a change of direction. We now have great data for our most vulnerable and high priority sets of patients — the patients who each have personal eligibility for both Medicaid and Medicare — and it’s clear to see when you drill down in to layers of that data that the differences within those dual eligible sets of patients between the ones who have joined plans and the patients who are simply on their own in the world of fee-for-service Medicare are huge.
The approach of patient focused care improvement exists and works now for those members because the plans are paid capitation and that payment model gives the plans very strong and very real incentives to look at how to change future cost trajectories for each patient and then gives the plans the opportunity to use the money made available by the capitation to actually put those differences in place for their actual patients.
We can look with today’s data flow at the clinically complex diabetes cohort of those patients and see obvious and extremely important results. We know that putting in place the right care for patients with diabetes related cellulitis, ulceration, osteomyelitis, gangrene or immediate and current amputations is very important to do because it changes lives and Medicare Advantage does exactly that.
No one debates the fact that Medicare Advantage patients have much lower use of hospitalizations, much lower use of emergency room visits, and much higher levels of care coordination for their care.
People with those same diabetes related cellulitis conditions are enrolled in the plans and because the plans are capitated and because the capitation cash flow has the plans benefit financially when those crisis and those expensive damaging events do not happen and because the plans can use the capitation money to build, hire and then use the care teams needed to reduce those damaging trajectories on a patient specific basis, the plans are currently turning that 17 percent who are at high risk in fee-for-service Medicare into 8.2 percent of those patients at high risk today, and the Medicare Advantage plans have both much lower costs and better care because that has been done.
That isn’t magic. It’s competence. Changing many of those care trajectories for patients is relatively easy to do if you have or create or build any kind of process at all in place to do it and if the caregivers for a set of patients are intentionally and directionally sent down that path and then supported in doing it.
It isn’t good or fortuitous happenstance or even good luck at some level for those patients. It’s basic blocking and tackling for Medicare Advantage Plans for some very obvious opportunities that exist for those patients — and the very sad truth is that Traditional fee-for-service Medicare does not do team care and completely misses those opportunities for almost every patient who needs them and their patients are damaged and often have harder lives as a result.
Fee-for-Service Medicare Providers Can Make More Money with Bad and Failed Care
We need to call that payment reality and that dysfunctional economic situation exactly as what it is and we should be both honest and clear in what we say about it.
Fee-for-service Medicare far too often delivers inadequate and even functionally deficient bad care and often ends up with completely uncoordinated care for those patients and because those fee-for-service Medicare caregivers are literally only paid only by the piece — the unfortunate and almost ironic and very perverse reality is that those care sites with bad care often actually get to make more money from their failure because the fee-for-service care sites get to provide more pieces of care when their care fails and they get to bill those pieces of care for that failure without any questions asked to Medicare and Medicare pays them.
That payment model enables and very unintentionally directly encourages too many of those outcomes — and it makes sense that we get those bad results far too often across our patient population when you think about how the payment process functionally works.
The car industry would probably have different design components if the manufacturers were paid more money when their cars crashed and if they were paid even more money for each car if someone died in the accident. The car companies would never design cars to kill or damage people for core ethical reasons but their current design and productions priorities would probably not focus as obsessively on safety, as they do now, if we were using that payment model and if we had that economic reality of paying more for accidents as the way we buy and pay for our cars.
The pure fee-for-service care sites all have very high ethical standards and the fee-for-service care sites would absolutely never ever do anything to damage or hurt any patient, but it’s also true that they tend to do almost nothing to change many care trajectories to improve performance in those areas.
The fee-for-service Medicare sites do not tend to have very many outreach programs to effectively reduce the number of asthma crisis for their patients or to reduce the number of heart failures in their patients in any effective ways for very many patients in very many settings.
They do almost criminally inept and inadequate work in far too many settings and care sites on not preventing amputations. The number of amputations is increasing in America.
We now have an $80 billion expense for amputations. We have an average of 230 people in America losing a limb every day at this point in our history. The cost of that care is added up and it is included in the average cost of fee-for-service Medicare in every county that we use as a foundation every year to build the new capitation levels for the Medicare Advantage plans.
The plans get to bid each year against the average cost of fee-for-service Medicare in each county to set their annual capitation levels. Those average costs for fee-for-service Medicare in all of those counties include all of those amputations.
That explains some of the Medicare Advantage surpluses that are created in the counties. The plan expense level calculation that occurs each year to see if the plans generate any surplus from their capitation and have to return money both to their members and to the government before taking a profit as a plan obviously has much lower level of amputation costs in it because the plans all deliver better care to those patients and those costs aren’t there for annual expenses for the plans.
That’s why the plans tend to bid capitations that are consistently significantly lower than the average cost of care for Medicare each year — because they have contractually limited profits and they would not be able to keep the surpluses that would occur just from matching their care costs to actual Medicare fee-for-service payment expenses in the counties and then keeping the difference. The bids tend to bid from 10–30 percent below the fee-for-service average costs in each county for their capitation level.
That bid far below fee-for-service average costs is another reason that the annual upcoding accusations have been so off base for so many years — because the plans can’t use all of the available cash flow now and it would be nonsensical, irrelevant and economically pointless to have those numbers coded higher. The plans already have significantly lower use of all of the hospital uses for their chronic care patients, and that’s what creates the surpluses that have to be distributed every year.
Various plans do their own discovery and invention processes in each of those areas and you clearly see those very intentional and well-designed programs in targeted areas — and that entire effort results in care teams doing things to reduce asthma crisis and heart failure crisis for patients in every Medicare Advantage setting.
When those hospital admissions for those conditions and those patients don’t happen, that lack of a bill for that care actually does reduce the $4 trillion total expense for America by the unbilled and the unfilled cost for those pieces of care.
Capitation paid to plans does go into that $4 trillion macro expense — and it’s a much better and more controllable way to buy care because the capitation payment allows for far better care and less expense in total on the care and that supports a slowing of the overall amounts being paid into the $4 trillion expense today.
Capitation is a very good way to pay for care when you understand how to do it and when you get full value for the dollars spent in that approach.
That pattern of better care delivered for those conditions is true in all of those settings because Medicare Advantage plans have a much better, more aligned and more effective payment model — where the plans are all paid by the month for each patient and where the plans are not paid by the piece at any point in the process for any element of care.
Very few health care policy researchers and health care economists ever write about that model or even reflect and mention that it exists — even though it is having a bigger positive impact on health care costs and on several layers of health care quality and processes in its Medicare Advantage model than any other payment approach being used in buying care in this country today
That fact and that process and those incentives have not been part of the community dialogue about Medicare and Medicare Advantage, because the financial and functional thing that almost all academic settings and all policy teams and a very high percentage of journalists who write about Medicare Advantage do not understand or even suspect at any level is that it is much cheaper to provide better care when better care means that you reduce overall costs and payments by reducing the most expensive care expenses — like asthma attacks, intensive care for chronic condition crisis, and issues like amputations and blindness — and the actual business model for Medicare Advantage today is anchored on and financially rewarded by that reality so the plans actually profit when they succeed in those areas and the rest of us benefit from what they do to create their profit.
Most Amputations Should not be Happening — and Fee-for-Service Medicare Rewards Medicare Caregivers Financially When They Happen
It’s actually easy to understand and to believe the link between better care and lower cost when you see what it actually happening for a couple of high volume and important key areas of care where better care reduces costs significantly.
Amputations are on the top of that list.
Amputations are a huge expense for Medicare. The Medicare fee-for-service hospitals and fee-for-service surgeons make significant amounts of money from every amputation. Amputations cost us, on average, $100,000 per patient, and they happen to patients so often that they now cost the nation through Medicare, in total, more than $80 billion a year.
Why is capitation relevant to that expense and to that pattern of care?
The Medicare Advantage plans are pre-paid their monthly capitation as their total revenue stream, so the plans don’t make any additional money by having people’s legs amputated — but the Medicare Advantage plans do all benefit financially when those amputations are not needed for any patient. So they are both incentivized and resourced to do very basic things to keep them from happening and they use the kinds of process engineering that improves products and improves processes in every other industry.
The 20-20 Pattern of Amputations is Important to Medicare Advantage Plans’ Process Thinking Reality and Approaches
What the plans all know about that particular topic is that in our country, 20 percent of Medicare diabetic patients are likely to have leg and foot ulcers as the result of their diabetes. What the plans also know is that 20 percent of those ulcers for those patients in this country currently tend to result in amputations.
That 20-20 is a relatively dependable, predictable and consistent long-standing pattern for relevant sets of patients and the long-standing functional reality for that process is that the plans can plan on that pattern happening for their diabetic patients as they look for opportunities to engineer care and to reduce costs.
When care is purchased by capitation and not by the piece, and when plans routinely do systems engineering and process thinking about care improvement at multiple levels, that particular 20-20 pattern creates a major and immediate opportunity for plans because they can clearly save millions of dollars by first reducing the number of patients who get ulcers and they can save even more millions of dollars by helping the patients who do get their ulcers and by doing what needs to be done on a patient specific basis of keeping the patients who do get those ulcers from needing amputations as the result of the ulcers.
Most of the health care academics and most of the policy people who write about Medicare Advantage today do not know or even suspect that type of cost changing opportunity exists for Medicare patients, because those opportunities are never mentioned in any of the thought pieces, opinion papers or in any of the economic and policy over view pieces in any way, even though they are a functional tragedy and a clear and unnecessary failure for care delivery and also extremely expensive.
The experts writing in those areas sometimes write about the possibility and even the danger of some coding issues for Medicare Advantage plans and a significant number of those writers even mention the specific diabetes diagnosis as a danger area for coding in some of those risk level discussions because MedPac has mentioned it more than once as a credibility threat in the coding process and other critics have followed their trail into that strange set of conclusions.
The people who have criticized and even attacked plans for diagnosing too many diabetics clearly have no clue that you can change a major cost item for Medicare across the board for all patients by billions of dollars just by knowing as early as possible which diabetic patients have feet that are becoming higher risk ulcer territory and by then doing the right thing for each of those patients to keep those ulcers from turning into lost limbs. You can’t do the right thing for each patient if you follow the Medicare Advantage critics strong recommendation that the plans not look for diabetics because their diagnosis codes might increase if that happens.
Everyone who runs a health plan knows with great clarity that those opportunities exist to improve care in all of those areas, because those costs and those opportunities are so important financially to the capitated plans and because doing practical things to reduce those costs can be a key part of the Medicare Advantage plans’ financial success.
It’s pretty basic process improvement done by the plans. The functional reality is that if you put the right processes in place to first know which patients you have are diabetic and if you then put simple and basic processes in place on a patient specific basis to both prevent the occurrence and existence of ulcers and then to detect them when they do happen at the earliest possible point in the ulcer process, and then if you focus on every ulcer that does happen and if you then do the right thing to keep that ulcer in each patient from triggering an amputation, then the plans can do that set of basic lifting on each part of that process as a care system and then the plans can cut the number of amputations by half or more by doing that work and they can save millions of dollars by simply doing those steps for those patients.
That happens. It obviously happens every day for large numbers of people. It’s an $80 billion total expense and it costs $100,000 for each patient. Plans generally want to change that huge amputation expense number and they want to reduce that major cost from both ulcers and amputations, so the plans tend to take advantage of that opportunity and they do it in systematic ways that begin by identifying every diabetic patient as being diabetic.
Plans that manage that care well look carefully at every diabetic patient to see which ones are having something that looks like it might be or become an ulcer in order to intervene with those patients as early as they possibly can in the process to change the ulcer’s status for that patient for the better.
Look at any Medical journal or Medical text book on ulcers and on diabetic amputations. The opportunity to have a major impact on their development and progression is clear if you look at that kind of medical data to find opportunities to improve care and then actually use them.
You can cut the numbers of ulcers that require amputation by more than half relatively easily by helping each of those patients with foot ulcers in direct and individual ways. Medicare Advantage Diabetics have far fewer amputations and the plans save a lot of money and save more than a few lives by doing that simple process and that all reinforces and utilizes and the business model that is funded by the capitation.
The overwhelming majority of economists who write about or study Medicare Advantage plans obviously do not understand the link between care improvement, care quality and the direct costs of care, because they don’t write about those issues, and they should now, as functionally newly enlightened economists, also see and understand why and — if need be — admit that that set of basic science and care approaches been rarely used in fee-for-service Medicare to cut any of those costs or to change those outcomes for very many patients in spite of the obvious needs for those changes to happen for their patients.
That’s why this piece calls failure for those patients a “shameful” metric.
The policy people and the economists looking at those patients should know the full impacts of those procedures. Fee-for-service Medicare providers can collect $100,000 when those amputations happen. Standard Medicare challenges nothing in the care process for any of those care sites creating that sometimes shameful outcome.
The economists and health care policy people who think about Medicare should remember and know, for their own context thinking, that treating foot ulcers more effectively to reduce the number of amputations is absolutely not new science at any level.
That information about those care patterns and the fact that we can reduce amputations in diabetics significantly by doing better work with ulcers in diabetic patients is valuable and visible old science that is finally being used now in a more consistent and more systematic and more beneficial way in larger volumes for the first time only because Medicare Advantage plans are capitated and because the capitated plans getting their cash through that business model have multiple economic and functional reasons to use those powerful and simple care enhancement approaches for their patients.
What is sad — and what should probably be morally unacceptable to us as a nation — is that the amputation problems are getting worse today for older Americans and our community health status is deteriorating in far too many settings because this is true.
The situation for those patients is actually getting worse in many traditional fee-for-service Medicare settings for those most vulnerable patients. Look at what is happening and being done in the country and in fee-for-service Medicare to deal with those ulcers for older patients and you can see from several studies that the care is deteriorating in far too many settings relative to the amputation trajectories and we are being warned clearly by very credible people that more people are going that terrible care situation and we should be doing something about it.
If you are old and if you are low income and if you have many challenges to face in your life today, then we should not collectively be have having your foot cut off added to your burdens and to your wrongful situation.
Amputations are not alone in creating that kind of failure and opportunity for us as a society and as a care system.
We need health care policy people, academics, and media people to recognize how many other care conditions have that same pattern of under delivered care improvement opportunities and we should get people to know how many enrolled people are being helped by Medicare Advantage and are being badly damaged in other settings by what we are not doing for those patients in those settings.
That condition is not alone in being a case where slightly better care done in systematic ways by science reinforced care teams can have a significantly lower cost and high value impact for patients that we are not doing. Diabetes is the most expensive part of the Medicare cost continuum, and several of the other highest impact opportunities are also happening there.
People are Going Blind who Should not be Going Blind
We tend to be public opinion cowards and we tend to suffer from extreme political correctness and from deep seated community positioning timidity, because people in our country do not want to criticize basic Medicare in any way.
Medicare might be the most popular program in the country by many measures, and it deserves that recognition and respect because it covers all of us as we grow older.
The truth is, however, it is not perfect. Looks at the data. We know that people are going blind because traditional Medicare is not doing what it should be doing for all of the relevant people and the fate of each of the people who go blind is to be blind forever because too many of us were cowards on raising those realities for the public discussion in a way that improved their care before going blind.
Medicare is doing some very good things that we should encourage with some of the ACO programs that do look at those issues, but the majority of the people who are at risk of going blind in fee-for-service Medicare are still losing their sight and we probably owe those patients some kind of apology for letting them be so damaged in that way for the rest of their lives.
Many of the people with amputations are owed that same apology.
Blindness should be a target and opportunity for us to make care better — and we are not doing it outside of Medicare Advantage. We all need to look at the fact that far too many people are literally going blind and those numbers aren’t shrinking.
Diabetes is currently the number one cause of blindness in the US. We have some of the world’s worst blindness rates for our older patients today and the cold truth is that the high blindness rates in America are overwhelmingly linked to diabetes and not getting care that should have happened for those patients.
This is another area where absolutely sold and useful old science hasn’t been used for far too many patients by fee-for-service Medicare in any structured or effective way. Managing blood sugar for diabetics is one of those areas where we have known what to do on a very important issue for a very long time and we have done it right for far too few patients, and we have the highest rate of blindness for the world for our older patients because of that failure.
Managing blood sugar levels for patients is an anchor to the process-related opportunity that exists to reduce or prevent blindness. Multiple studies have shown everyone for a very long time that you can cut the blindness rate in half or more just by managing the blood sugar levels of diabetics.
Blindness is expensive, devastating and damaging for many life issues and situations, and it is just plain wrong as a health outcome for us and for our people that we have growing blindness rates in our country because it is clear that we actually can prevent it for so many people.
The Medicare Advantage five-star plan for quality makes diabetes a focus condition, but that focus on better care would have happened for those patient enrolled in Medicare Advantage plans just based on those many opportunities that exist to help diabetics and to simultaneously reduce the cost of diabetic care.
Medicare Advantage plans know the science and the opportunity and they also know how much money they can save by getting people down the right path that does involve the levels of care that people need as they go blind. Because the plans are capitated, they have the money in their flow of cash to put in place the levels of systematic care for diabetic patients that create much lower long term and immediate cost levels for those diabetic patients and save vision in the process.
For the Special Needs patients with co morbidities, the plans develop patient focused care plans and they make sure that they get the right care to every patient every day as needed and have extremely good patient centered processes in place for everyone.
None of that care is happening for the traditional fee-for-service Medicare patients in any systematic or organized way.
The cold truth and the sad reality is that Fee-for-service Medicare far too often hugely fails diabetics at multiple levels and the patients suffer the consequences of that inadequate care.
That isn’t even up for debate as an assessment of relative performance levels between the two funding approaches that pay for most care for America. Fee-for-service Medicare does not do what needs to be done in most settings to cut the blindness levels for diabetics. The tools and processes aren’t even there in too many of in those settings and too many of our fee-for-service care sites don’t even have any combined medical records for our patients that identify who would benefit from that care.
Fee-for-service Medicare care sites also often have weak, inadequate and unlinked medical records — and the unfortunate reality is that those many of those care sites far too often don’t even know which patients they have who actually have that disease.
They inherently do the exact opposite of upcoding — and one of the interesting aspects of the attacks from some of the Medicare Advantage critics is that they refer to that information deficiency in those sites with approval as the norm for patient record keeping and some of the Medicare Advantage critics even seem to both defend and prefer and even protect that completely inadequate record keeping approach it as an acceptable approach to care information collection.
By huge contrast, Medicare Advantage plans immediately look for diabetes in every patient because that information is so useful at so many levels. The Medicare Advantage plans all know which patients are diabetic and the plans consistently have patient specific plans in place to both manage blood sugar and to look for early levels of foot ulcers to keep them from turning into amputations and also to help manage their other co morbidities in intentional ways to reduce the rates of mortality for those patients.
Deaths are prevented at significant levels by the Medicare Advantage co morbidity work for patients with multiple conditions and the care coordination that exists in the plans for those patients.
We Need to Get People to Plans Where Everyone is Above Average
The plans are not all perfect in all of that work but they are all so much better and they are all so much more consistent and more effective than fee-for-service Medicare in most settings in helping diabetic patients that we need to start thinking and discussing as a country that it might be an ethical issue and a moral failure for us as a country not to more intentionally steer relevant people away from those settings where they lose their feet and where they go blind and we need to get them before it is too late to Medicare Advantage plans where everyone is above average.
MedPac has said clearly and often that they oppose steering patients in any direction. They explicitly say and they clearly think steerage from MedPac is wrong.
MedPac staff and writers are very careful not to point out or mention or even notice the obvious and clear quality failures of fee-for-service Medicare that give us more blind seniors than any western country because the MedPac staff does think sharing that information in any direction is not fair to the fee-for-service Medicare program and they make fairness to that program a goal.
That is bad policy. MedPac should change their approach about steerage because we do have more amputations than any other western country and they are happening for real fee-for-service Medicare patients who have no one looking at their foot ulcer treatment and processes and steering them to care settings that will support them in having better lives.
As a nation, we should be looking at all the things we can do to get that information about relative care outcomes to patients. The news media too often also has had no clue on most of those quality and performance gap issues, and we should encourage a new level of medical enlightenment for the media that includes care improvement as part of their agenda.
The Media are missing a plethora of very legitimate stories about what is happening in health care quality efforts. They could write stories and do reports every year celebrating which local plans have achieved five-star status on the Medicare Advantage rating system to tee up those reports and they should ask the care sites with four- and five-star ratings to celebrate their internal local successes in those quality and service areas and to explain some of the solid things being done in those settings to make care better and more accessible to their patients. The public would love to know that some plans are doing some very positive things to make care better and that is legitimate news to cover.
The patients will benefit from those stories and those hero stories will encourage other care sites to do similar programs and stories.
When the plans achieve those ratings, the local media should describe those successes because they are real wins and because they can create public expectations for care improvement by the other plans and patients.
The news media and the health care publication and services should also be looking at those sets of failures of care, and the media should be informing the public about those issues and about those dangers rather than taking the fake bait of MedPac and their staff who are still writing about risk coding levels for health plans as though the business model of plans actually is to refine their actuarial and coding skills and not to improve their care.
Real people’s lives with Medicare coverage are being damaged because they are not in the best patterns and in the best approaches for their care. People’s lives are damaged and sometimes even ruined by those kinds of health outcomes in so many settings.
The Medicare Advantage critics who actually wrote recently in a couple of critical documents that ran in credible policy settings that the Medicare Advantage plans literally only collected diagnosis information about diabetics so the plans could “upcode” their risk levels for payment purposes for those patients should now apologize.
They said it more than once.
It is not true.
They owe an apology to the world for misleading people so badly on such an important point of fact about why plans collect information to discover who is diabetic. That accusation in credible settings has caused some relevant people to have less faith in plans. One very critical piece also said that the plans who sent the nurses into homes did it purely and only so the nurses could “harvest diagnosis” and not to deliver care. That story was also clearly extremely wrong at multiple levels — and it has been repeated in multiple settings.
The plans, in the real world, obviously very quickly gather the information about which patients are diabetic because that is extremely important and useful information for providing care to diabetic patients.
That entire array of processes to improve care and to reduce future hospitalizations for people with all of those chronic diseases were designed, were built and exist now in all of those settings only because the Medicare Advantage plans are capitated and because the business model of capitation thrives on volume and on getting rid of reams of unnecessary costs in all of those areas.
The current data shows us that the plans can and do very intentional patient focused work that can cut the very worst care outcomes for many categories of patients and those approaches exist for each plan in significant part because the plans spend less money when they succeed.
Cutting Congestive Heart Failure Crisis by Almost Half also Keeps Patients Alive Longer
Congestive heart failure is a particularly good example of how that cash flow and financial flow works extremely differently for fee-for-service Medicare and for Medicare Advantage and what happens to those patients directly reflects how each way of paying for care changes how the care is delivered.
Congestive heart failure kills a significant number of people, sometimes far too quickly. It’s painful, life threatening, often frightening, and it can make a major negative difference at many levels in many people’s lives for a very long time once it begins to change a person’s life.
Medicare Advantage plans do the right things for those patients using their capitation payment cash flow to fund each right thing.
Medicare Advantage plans very intentionally discern and detect who is at high risk of having those kinds of Congestive Heart Failure crisis events and the plans very consistently intervene on a patient specific basis with each patient to manage the risk and to avoid the damage for those patients.
That tends to be a profitable condition for fee-for-service care sites.
The fee-for-service Medicare care sites make significant amounts of money from each congestive heart failure crisis. The hospitals get paid $20,000 to more than $40,000 with no questions each time one of those crisis happen for a patient, and that is often very profitable care delivery for those sites.
Their marketing teams at those fee-for-service Medicare care sites work hard to get as many referrals as they can for those patients from other fee-for-service doctors in their area. The care sites don’t do things to reduce future patient damages and current risk levels.
Very few of those fee-for-service programs who make $20,000 to $40,000 from each damaged patient do very much to prevent them from happening in the future. Those care sites very consistently do deliver great care to the patients when the crisis actually happens, but they don’t do much to avoid them or to keep them from happening.
Capitated Medicare Advantage plans reduce those admissions by over 40 percent in most settings. They set up very specific care plans for each patient, and they assign care team members to those efforts to help the plans succeed.
That’s the genius and the beauty of capitation. The plans take their capitation cash flow and they use part of it with no challenges from Medicare to invest in in those processes that can help to keep the future crisis for each patient from happening. Nurses and other support caregivers are often part of the process and they often help get the patients out of risk and coach them into less damaging approaches.
Some plans have put very accurate scales into patients’ homes and some of the scales in the homes of the patients have an actual telephone link and that link can be set up to call the care team when the patients have unexpectedly significant and alarming weight gain that says they are in potential trouble.
Many emergency room admissions have been avoided when the care team detected weight gain of a patient triggers the right care and steers patients to safe places and better outcomes.
Traditional fee-for-service Medicare not only does not do many of those kinds of patient support activities that Medicare Advantage plans do, the reality has been that the traditional Medicare program has explicitly been very opposed to having those nurses in those in-home settings — and they can file legal action against any care site for what they call Medicare billing fraud if a nurse in that home for that patient bills fee-for-service Medicare for that care.
That’s another example of the differences in approach that often makes Medicare Advantage hugely better and safer care and those levels of flexibility in use of that cash flow to put the right people in place is why the capitation model is so useful in getting care outcomes to better places and to higher levels when you know how to use the process engineering tool kit for each condition well.
“Medicare for All” Should Insist on Using the Best Care
We need the people who are advocating for Medicare For All as a universal coverage program for the entire country to realize that the idea of universal coverage for everyone is a solid and good goal and it deserves support — but doing universal coverage with a payment approach that creates the highest level of older patient blindness and the highest volume of foot amputations in the western world is a bit suboptimal as a destination for everyone in the country that we should all want everyone to have.
Let’s raise our expectations for Medicare For All.
We should want Medicare for All to be patient focused and to use the very best levels of care and we should want the care approaches that are used for universal Medicare to be continuously improving as a strategy and a commitment and a goal, and a competency and a skill set because the American People deserve Continuously Improving Best Care and because we can clearly afford it because it will cost less than having too many hospital admissions for bad care.
We have more than enough money to pay a capitation that can make that happen and rationing anything in that process to save money to make universal coverage affordable for the country is both unnecessary and wrong.
The Affordable Care Act does not get the credit it deserves for transforming Medicare Advantage into a much better purchase for the country. The Affordable Care Act carefully designed and built the best features of the Medicare Advantage program as a care improvement and cost containment tool for the country and not as just another way to pay Medical fees for people with Medicare coverage.
The Affordable Care Act built several of the best care and delivery structuring features into the Medicare Advantage portfolio. Far too many people in our country did not see, understand or appreciate what they were doing when they did that because they didn’t explain what they were doing and the political and public discussions at that time were focused on other parts of the law.
The Affordable Care Act Redirected, Rechanneled and Refined Medicare Advantage.
The Affordable Care Act significantly refined, improved and enhanced Medicare Advantage. They rebooted the program, took it away from the sway of some of the early players and redefined it to be a purchasing model for care and not just a payment model for pieces of care.
They took the old program and immediately reduced some key costs that had some prior levels of over payment and rebased the cost levels. They also created intentional and important purchasing power through the contract for CMS over creating performance expectations in a number of key areas and their use of those enhancements have been responsible for many of the Medicare Advantage program success today.
The tools that CMS is using today to steer performance were intentionally built into the model by the Affordable Care Act and those improvements have the same kinds of long-term staying power as the somewhat parallel pieces and somewhat parallel requirements created for the Exchanges in every state that also very intentionally give people choices of health plans for their core coverage and their care and keeps them affordable for people who need them.
That very intentional and clear design role for Medicare Advantage from the Affordable Care Act is increasingly visible and it is increasingly appreciated over time because it has so many effective moving parts and it actually creates better care for less money as they intended to happen when they wrote that law.
Possibly the most important unexpected thing that Medicare Advantage has done for us as a country has been to provide a badly needed safety net for 5 million of our hard-working retirees who had spent their lives with employer based and union-based retiree health care benefits as their expectation for their care when they retired.
The challenging truth was that many of the trust funds and many of the retiree related health plans faced major challenges and some were seriously underfunded. Had they continued entirely under their own funding stream, up to 5 million Americans who thought they had assurances for their retiree health care could have been in serious difficulty. Having all of those people who had worked hard and who thought they had retiree coverage for their health care scrambling for enough money to pay their health care claims was potentially damaging to those people and to the country.
The Affordable Care Act created a safety net by setting up an employment-based set of trust fund coverage options — and we now have 5 million people with absolutely solid and guaranteed retiree coverage through Medicare Advantage. We actually now have Medicare For All with extremely good benefits for more than 4 million retired union members because of vision and the design of the Affordable Care Act.
That program is funded and runs at a pace with seriously contented members because their retirement expectations are being met.
The MedPac people who continue to attack Medicare Advantage are careful to leave that entire set of people out of their communications every year because they know how popular that program is with the retirees, former employers with health obligations and with labor unions with those programs in place.
We should continue to channel people into each of those pipelines for coverage and care.
We should also recognize that we have already begun to use it as the working foundation for Medicare For All if the Congress ever gets to the point of moving in that direction.
We also need everyone thinking about the care area to know and understand that those differences between fee-for-service Medicare and Medicare Advantage are very directly created by the flow of cash into each program and we need to understand that flow of money will continue to create those differences in each direction because that’s what happens in any industry when cash flows.
This approach being used for Medicare Advantage plans to change that trajectory for those patients isn’t rocket science. It also isn’t actuarial data manipulation or any level of economist formulae academic fine tuning. It’s simple functionality and process engineering and we now know that we can cut Medicare patient blindness by more than half by functionally managing processes and approaches that can steer the blood sugar level of each diabetic in the program to get them to the right levels.
We should obviously do it for every relevant person on Medicare because we know what it is and we know how to do it.
In fact, not doing some of that care improvement work now for those actual people who are in the fee based Medicare program is so wrong that its almost an ethical issue for us as a community because real people are going blind when we don’t make sure the basic care is being done for them and we should think of it as a huge and even shameful ethical failure for us to allow that many people to go blind today and to accept that as a macro purchasing failure for Medicare fee-for-service care cash flow and not look at the ethical consequences inside that package for people’s lives.
We have massive opportunities for diabetic patients, because they are almost half of the Medicare cost burden and because we now know so many functional things that can make their lives better.
The Medicare Advantage five-star quality agenda includes diabetic care as a target area for obvious and highly valuable reasons. Even during Covid, the blood sugar levels for those Medicare Advantage patients improved by almost 2 percent.
Health care academics and health care policy people need to expand their paradigms to recognize and understand that bad care is very expensive and it also functionally hurts and damages people in what should be unacceptable ways to us as the purchaser and payer for that care.
We Americans need to raise our expectations — and then we need to intentionally pay for what we expect to happen in ways that actually cause that to happen. Medicare Advantage does exactly that by setting clear and continuously evolving expectations and using their leverage to improve care.
The specifications on care and service that are built into the Medicare Advantage program are good and solid, and they get better every year. As intended by the Affordable Care Act, CMS functions today in very real ways as a buyer — not a payer — with that system and you can read what they are actually now demanding and mandating now in exchange for their capitation payments for 2023 operations below:
The 2023 Expectations for Medicare Advantage from CMS have Several Excellent and Powerful enhancements
Please read this:CY 2023Medicare Advantage and Part D Proposed Rule (CMS-4192-P)
Everyone wondering where Medicare Advantage is going now should read those very specific and explicit requirements from CMS that they have created as a demanding buyer for the plans for next year. The leaders at CMS go through a similar process every year and you can learn a lot about the program and what it does from the expectations they set for it in that annual document. The old sets of those documents are worth reading for context and direction and a sense of their mission.
The current expectations are both very real and important, and they are creating the kind of care for their beneficiaries that we all should want delivered to the people we care for, respect, and love.
That program has been fiercely attacked by people who generally don’t know what it does or what it actually is but who oppose it and resist it for their own set of ideological, political and. sometimes, financial gain, or economic advantage issues and reasons.
Misinformation about Medicare Advantage is created far too often by those critics and opponents with great enthusiasm and energy and an almost total absence of actual functional data or understanding of what is actually happening.
That set of attacks on those agendas is bad for the country because it is so inaccurate. This is the wrong time for us to have inaccurate information about care because we should be building great care starting now.
Our Goal Should be to Build on the Golden Opportunity We Have for Great Care
There is far more at stake than just getting the prices right for Medicare.
We could and should be on the cusp of a golden age for care that uses a combination of care connectivity processes, best science, artificial intelligence, patient focus and continuously improving disease detection and anticipation tools that will make care much less expensive and far better at multiple levels.
The core process of Traditional fee-for-service Medicare has always resisted that set of tools and they resist them with conviction because when you only buy care by the piece, you need to worry about adding more pieces to the mix without knowing what they might do to the cost mixture for those patients.
Medicare Advantage will obviously use the new tool kit and plans will compete to be there for their customers and patients with those tools — both to attract additional customers and to bring down the costs of each piece of care for the patients they have.
When Medicare Advantage does electronic patient visits, that is much better and more interactive care and it has the potential to be the new normal for all care. During Covid, some Medicare Advantage care sites got up to 80 percent of their visits with electronic connectivity that the patients often prefer. Fee-for-service Medicare initially banned it, and is reluctantly now trying to figure out how to meet patient’s expectation in that area and still kill those connections because patients love it and many caregivers find that they can deliver better care for many patients when they are electronically connected.
We should set up a context for great care — and it should be great care that very directly meets the needs of our lowest income beneficiaries.
Two out of Three Low-Income Medicare Members are in Plans Today
Enrollment in Medicare Advantage is growing nicely and it is relatively stable over time. Roughly half of our Medicare beneficiaries are now in plans and that total number of enrollees grows slightly every year.
It covers about half of the Medicare people now.
We need to know and understand who has chosen what as we go forward with the program.
The people who have stayed with traditional Medicare through multiple opportunities to enroll in plans tend to be higher income people who have longer term relationships with the own personal long-time care sites. Their net worth is more than $100,000 over the groups of patients who are actually joining the plans and many have been getting care from care sites for higher income people in the past.
Most people hate to change doctors. It can be very hard to change doctors when you are happy with your doctor now. Many higher income Medicare Beneficiaries have those good longer-term relationships with their physicians and many of those more satisfied patients will probably be loyal to traditional Medicare for a very long time for those reasons.
That is not our most diverse set of Medicare members. Only 16 percent of the traditional Medicare enrollees are minority members today.
By contrast, our lowest income members and our largest groups of minority members have overwhelmingly become members of plans.
Two out of three of the lowest income Medicare members have now joined the plans.
Many of our current lower income Medicare beneficiaries don’t have those long-standing and positive linkages with care sites and many of our lowest income Medicare beneficiaries do not have any of those kinds of relationships at any level with their local doctors or local care systems. Many of our lowest income beneficiaries live in settings where those sets of doctor availabilities and relationships do not exist at high levels, so the Medicare Advantage plans are their easiest, fastest, and, for many, possibly their only possible access to an actual direct relationship as a patient with a care site or a care team.
Over half of the African American members and more than two-thirds of the Hispanic members have now joined the plans, and they have had very high satisfaction levels with that choice.
Many of those patients from those groups and settings now have a personal doctor and a patient focused care team for the very time in their lives. That is much better and more personalized care, and patients tend to appreciate getting it.
The satisfaction numbers for the new and current members is currently very high.
We have extremely solid support among the members at all income levels for their plan links and we also have very strong support with Members of Congress for Medicare Advantage right now because the members of Congress hear from their constituents, and they can see that their voters like the plans and they can see that their voters have better benefits for less money.
The Medicare Advantage program costs significantly less than fee-for-service Medicare in most counties. Critics of the program try hard to pretend that isn’t true, but the plans all have lower costs than the average costs of fee-for-service Medicare in every county, and those lower costs are permanent savings for the Medicare trust fund because the capitation cost is the only money the government will ever have to spend for the plans and it is being paid every year at capitation levels that are lower than the average cost of fee-for-service Medicare in each county.
The plans have expenses for their members that have to be paid for from the capitation. The plan expenses are totaled annually to see how well each plans did financially each year.
If the expenses from the plans are higher than the capitation, the plans eat and absorb the losses. There is no way for the plans to be ever be paid any money from the Medicare trust fund beyond the capitation payment.
If the plans expenses are lower than the number created by average cost of Medicare in those areas, that creates an internal cash surplus for the plans that is used in the ways that the program set up to benefit both members and plans.
The plans have both legally limited profits and a clear path for sharing the surpluses they create with their members. The surpluses must be shared with the members and that sharing with the members allows the plans to have much better benefits than fee-for-service Medicare in all of the counties and to have lower costs for many areas of care.
Those surpluses in each of the counties that shared with plan members are everywhere — and those surpluses might higher this year because CMS has looked at how much the plans could be paid based on their current enrollment and relative risk levels from the encounter reports, and they have raised the potential payment level from CMS by more than 8 percent for next year.
The plans clearly will not be able to use that additional money to increase their profits because their surpluses are at top levels now. It will be interesting to see what the plans decide to do their year on pricing and capitation and benefit expansion to respond to that additional money.
Major critics of Medicare Advantage plans have been arguing that the old cash flow was based on plans doing clever and sometimes unethical things to increase their risk levels that triggered their cash flow. “Upcoding” has been a major accusation for the plans for many years.
The people who have been complaining in a number of settings that Medicare Advantage was badly over paid and that the cost levels of fee-for-service Medicare in the counties that triggered the first round of data for the capitation process in recent years was wrong and being wrong was caused in some unclear way by Medicare Advantage plans doing upcoding of some kind are completely wrong and their accusations are now even non sensical because the coding system is actually gone.
The higher capitation availability levels that the critics and opponents have said were somehow created by plans doing serious and inappropriate upcoding were actually based entirely on the fact that the average cost of fee-for-service Medicare in our counties today is so high because it is bad care and bad care is very expensive.
The plans did not inflate their risk scores because they did not need to create wrong risk numbers to justify higher costs when the average cost of fee-for-service Medicare coverage in each county was so expensive because so much of the care has been clearly bad.
The much higher rate of hospital admission for congestive heart failure with the fee-for-service Medicare payment approach is in the county totals and that expense creates a cash flow that it is extremely easy for the Medicare Advantage plans to beat.
The amputation expense of $80 billion is included in the average county per capita costs that created the first cost levels each year from the Medicare fee-for-service expenses. None of the plans are doing amputations at that $80 billion level, so the amount that is the expenses that they use to see if they have a surplus is based on whatever their current amputation level is.
That’s better care. Not upcoding.
The upcoding accusation was highly flawed and it is now completely impossible because CMS actually eliminated coding for the plans two year ago. No one can upcode now because no plans today can code at all.
CMS now collects information from each and every patient encounter — so they now know what the diagnosis was for each piece of care and they know what the procedures were for each piece of care. That is extremely accurate and very current information — and there’s no place like the old plan coding profile for plans to even suggest codes.
This would be a good time for us to move away from that old and disruptive set of debates about risk coding and move on the a far more productive discussion of how we can create great care for all Americans and do it with less money than we spend now.
We Should be Building an Incredible Array of Continuously Improving Care Tools
Care can be hugely better and that should be expanding and improving Now.
Great tools are being built. We need to use the full possible tool kit being created today to deliver what should be continuously improving care with better outcomes, better processes, and better cost levels because that happens in most industries when you engineer the products well. Care is obviously on a trajectory that could and should get to that result.
Artificial Intelligence is exploding as a powerful and game changing care support tool and it will continue to explode.
Very amazing new tools are coming into existence — and they will be used by Medicare Advantage plans early and well because the plans have a major financial reward associated with that can be linked to reducing the crisis level of those events.
Medicare Advantage plans lead in several of those technology areas now and they will enhance their leads in all of the new high-tech care support because the tools are better and the capitated plans have major financial reasons to make care better because the new tools will enhance care and most will do it for less money that they spend now.
It will be much cheaper for care delivery and for the Plans to actually know with more than 80 percent accuracy which patients are likely to have a heart event next year — and the plans will use that data to change the trajectory and the reduce the costs for that event while creating better outcomes.
The organizations developing those very real new tools will be competing to make them available — and the plans will be competing to get access to them and to use them.
Fee-for-service Medicare will fail completely in using those tools.
Traditional fee-for-service Medicare isn’t even in the technology improvement game at any level. That has been their clear choice. Traditional fee-for-service Medicare has never been supportive of those sets of tools and they are not going to be changing their approach to innovation now.
The reality is that traditional fee-for-service Medicare won’t even pay for any of those new tools for a very long time — if ever — so their patients will get inferior care in all of those areas and their patients will continue to be more expensive than Medicare Advantage because the reality is that stage four cancer is much more expensive than stage one cancer that is detected much earlier for most patients by the new cancer detections tools. Far too many fee-for-service Medicare cancer patients with be diagnosed at stage four while the Medicare Advantage plans will all use the early cancer discernment and the early detection tools (just like they manage blood sugar to prevent blindness) and their cancer care will cost a lot less and will have much better survival rates.
Some of the new heart crisis detection tools can predict with more than 60 percent accuracy now from in home devices that an adverse health event will happen for a patient within the next 12 months. Plans will save a lot of money with that information because they will be able to intervene and respond extremely quickly in ways that are rewarded by the plans being capitated. Plans will be current on every one of those new technologies and many plans will probably compete in the market with their comparative access to those sets of diagnostic and intervention tools.
If a patient is trying to decide whether or not to join and plans and if one of the plans say they have a new blood test that will identify with better than 60 percent certainty that any of 50 cancers will or will not happen within the next year for them as a patient, that could be a good market tool for that plan and people will be likely to join the plan to have that advantage in their life and care.
The plans will have care teams attached to that flow of data. That’s far superior to having an application on the internet that creates a flow of information to patients that leaves the patients on their own in trying to figure out how to respond to whatever the information from that test or process reveals.
That isn’t speculation.
Many of those tools exist now and are being perfected. Medicare Advantage plans can get them to their members — and fee-for-service Medicare won’t have any vehicle for their use and will probably not pay for almost all of them.
Some People Still Say that Plans Have Inflated Profits Triggered by Inflated Risk Codes and That’s Very Wrong
The plan profits are limited by contract and the profits limited by law and the actual profits for Medicare Advantage plans currently average about 4.5 percent per member. The critics often lie in some documents, speeches and settings about the profit levels of the insurers and try to make it appear as those numbers are higher.
The 4 percent levels are not abusive profits, even though some of the most aggressive critics say they are. That’s less than half of the normal and average profit levels for American businesses, and it is very far from the excessive and exorbitant profit levels that some of the most negative Medicare Advantage critics claim repeatedly that the plans receive.
There are some critics who simply oppose having health insurance companies functioning as health plans and who say that any health insurance company who gets money from Medicare Advantage is simply getting a wrongful flow of cash.
It’s a combination of ideological, political, emotional and economic opposition, and it is hard to address if it’s actually ideological as a core component for the belief. The actual profit levels for Medicare Advantage plans are under 5 percent and that’s less than half of the average profit levels of American businesses and less than the profit levels of just about every other element of health care in America.
The drug companies all make more than 5 percent and even hospices are currently granted 9 percent profits by Medicare.
You can hate and oppose the use of insurance companies for whatever reason, but we can’t blame them for abusive profits in that space. The Affordable Care Act did an extremely good thing by limiting the profit levels and the administrative costs of all health insurance companies to 15 percent, and the plans can’t ever charge 20 percent profits in Medicare Advantage or in the insurance exchanges because there is no way around that very well-conceived and designed 15 percent limitation.
The insurance companies deliver high quality Medicare Advantage plans and many obviously do good work. The first two health plans in America to get tests to their Covid Patients were Kaiser Permanente and Optum, and they both did it weeks and months before anyone else was doing that work in any systematic way.
One is extremely not for profit, and the other has the biggest for profit cash flow in the business, and they both achieved that goal of getting Covid tests to all of their care sites for similar reasons.
So Plan structure and the role of insurance companies needs to be recognized as an issue that concerns some people, but it clearly does drive much that says this agenda isn’t the best for Medicare patients or is creating any damage to the process.
They are all motivated to create the same kinds of better care outcomes, and the bids for all are below the average cost of fee-for-service Medicare in all of the counties — and that means the Medicare Trust fund got a good deal with those bids.
The core strategies look alike in the plans regardless of their for-profit status as businesses.
Anyone who has managed to get to a senior leadership job in a capitated care system understands the basic business model and we know from decades of experience that the leadership of all plans is continuously looking for a growing number of ways to make those kinds of care improvement successes happen to create lower costs and better care for their members.
It isn’t rocket science. It’s actually remarkably simple work. We can all see exactly what happens and we all know the reasons for doing it.
It’s almost too simple as a strategy to be as effective as it is.
Care teams at plans learned long ago that quick weight gain is often a high value warning of congestive heart failure — so many plans have been known to put extremely accurate scales into some patients’ homes that have telephone connections. Those scales and phones are used to notify the Medicare Advantage care team if a patient weight gain seems to indicate they might be at increasing risk of a failure and crisis.
Many very successful interventions have happened from just that information.
Every other industry uses process engineering to improve their products and reduce their expenses. Fee-for-service Medicare engineers absolutely nothing and Medicare Advantage plans engineer wide ranges of things because they have the resources to do it and they are rewarded financially — in an optimal win-win total context — when they succeed.
Medicare Advantage is almost the only place in American health care where that set of interactions is the goal of the purchasing model and it actually happens.
There really is a lot of low hanging fruit because so much of fee-for-service Medicare is so consistently bad care. We should not collectively criticize or even condemn that set of fee-for-service Medicare caregivers that service so many of our patients. There are many great and wonderful and even underpaid caregivers in Medicare care settings and when you look at heroic care delivery and when you look crisis response performance for patients, the fee-for-service care infrastructure always steps up to the plate and they very often even deliver great care.
But the best care sites there have to step up to the plate far too often — and we owe it to ourselves to think about what directions we should be going as a country if those millions of patients are in crisis modes in hospitals 30–60 percent of the time more often than those crisis should be happening.
Medicare Advantage has Serious Critics and Opponents
There are serious long-standing Medicare Advantage critics who continue to attack the plans — with what are obviously angry and inaccurate and sometimes non sensical attack points. We need to respond with facts to every attack point and we need to work past those attacks by looking at what the plans are actually doing and convince credible people that the critics are wrong and Medicare Advantage is a very right part of the solution set.
The reality is very different than the attack points of the critics. The costs of Medicare Advantage are lower at multiple levels and that’s easy to prove because they happen in plain sight.
The bids from the plans are lower than the average costs of Medicare in the counties. The plans generate surpluses every year and the only way to generate a surplus is to be lower cost than fee-for-service in those counties. The critics say that even though the plan discounts in every county make it appear that the Medicare Advantage costs were lower everywhere — they believe that the plans have done some serious distortion of their cost levels by doing coding manipulations.
They argue directly that the plan upcoding process has distorted that conclusion about relative cost and some argue that that a plan upcoding correction of 9 percent needed to be added into the plan costs in all of those counties to offset that deficit and to show the real cost of Medicare Advantage.
But even before the new numbers, it was clear from the old numbers that Medicare Advantage cost less than traditional Medicare on a legitimate measurement basis in all of those counties.
A slightly more actuarial look at the costs from Milliman showed that in the year they studied, the average cost of fee-for-service Medicare was $1203 per member and the average cost for Medicare Advantage members was $1,055 and the plans clearly cost less money for very definite reasons.
The care is both better and less expensive.
Even the death rate from Covid was affected by having better care for those enrolled people. We saw early that for high-risk patients with multiple conditions the normal Covid death rate for fee-for-service Medicare patients outside of the plans was 22 percent and we saw that when each patient has a set of caregivers keeping track of their care needs and responding to them, that brought the Covid death rate down to 15 percent.
The worst place to be in the country early in the Covid experience was in fee-for-service Medicare because there was literally no response strategy from that program at any level for that disease. The people who argue that we should continue to support that program as our baseline care model should keep in mind that they did absolutely nothing for Covid patients.
That should not have surprised anyone.
That’s the same pattern as we see for all of the other conditions.
Follow the dollar.
Look at what CMS is requiring now of Medicare Advantage for 2023.
Our Biggest Care Success as a Country is Our Dual Eligible Special Needs Plans
The Medicare Advantage Special Needs Plans are special.
Medicare Advantage should be getting extensive credit right now for what has been an extremely important care delivery success that has helped millions of our highest-need and lowest-income patients in life changing ways and that has been almost completely invisible to everyone in the country.
The biggest area of success for us as a country on health care improvement and health equity right now is probably the extremely important work being done by the plans for the people who are eligible for both Medicare and Medicaid.
That set of people has the lowest-income levels and the highest health care needs in the country, and they have multiple serious health care conditions, and the Medicare Advantage plans are doing wonderful care and also saving money for that set of people.
We now have 4 million people enrolled in Special Needs Plans in Medicare Advantage. Those people have dual eligibility in both Medicaid and Medicare — and they actually do represent the lowest-income and the highest care-need portions of the older American population. They have severe and disabling chronic conditions and they often have needs for skilled in-home care.
CMS strongly supports that program and they are doing things to cause it to continuously improve.
They want that program to continue to exist because when you look at the care needs of those dual eligible people and when you compare them to the care status of people with the same economic status and health status levels in traditional fee-for-service Medicare, it’s obvious that the health plans do far better on care than the other care sites available to that set of people and that their success is on a sustainable path.
The work done with the dual eligible patients with multiple health care needs has given the caregivers in the plans an extremely important opportunity to both reengineer and improve care. Almost all care in America happens in siloes.
Caregivers don’t communicate with each other and medical information isn’t shared about given patients. The number of incorrect diagnosis is far higher than it should be and the level of care coordination between caregivers with multiple conditions is extremely low.
The very best super clinics do spectacular work in those data use areas — with Mayo Clinic and Cleveland Clinic and Kaiser Permanente having extensive information about each patient that they share with their entire care teams and get great results — but the vast majority of other care sites don’t have that level of patient support or care linkages and very few sites have the kinds of commitments to the next generation of best care that Mayo exhibits on a constant basis.
But — the Medicare Advantage plans all do better than the old model on care connectively issues and Medicare Advantage plans flow with that future model of connected and continuously improving health care.
The health plans who make up the Medicare Advantage care context have best care as their goal and they share data and care expertise and competence in systematic ways in order to maintain their market lead on the delivery of care.
Look at the extremely relevant and informative numbers in the chart below about the differences we see between patients in each of the two payment models. This isn’t ideological differences. These numbers result from actual care:
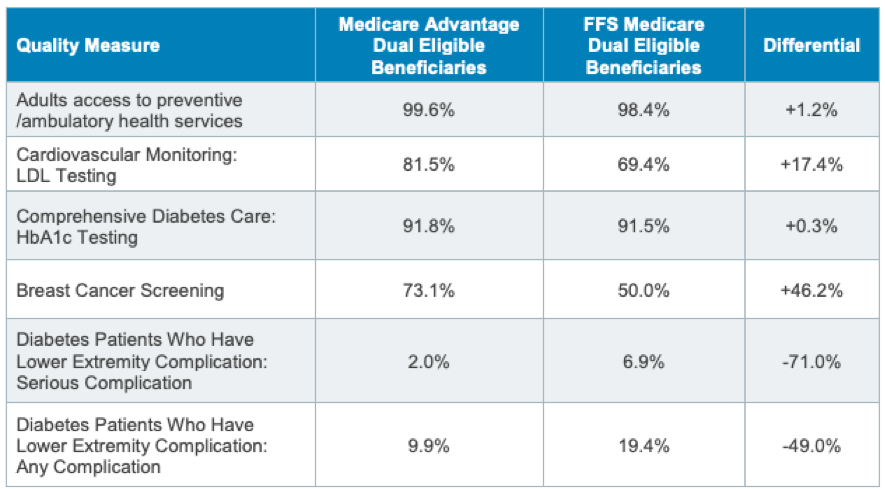
That much lower 2 percent level of people with diabetes who are facing serious complications today for their lower extremities is good for patients because it puts many lives on much better care trajectories. That lower number happens because Medicare Advantage is capitated and has the right cash flow to both fund the necessary care improvement processes and then to financially rewards the plans when it happens.
We should be ashamed of ourselves as a country when we understand those numbers. Every doctor and every care system in America knows the needed science for those key conditions. But that level of direct patient focused care has not been used for very many people in the past because the financial model of fee-for-service Medicare has been based on pieces of care and that payment approach changes how caregivers think about their priorities, practices, and processes for their patient.
The truth that most health economists hate to add to the discussion but one that we need to put on the table now for everyone is that in that fee-for-service care payment model is that some care sites and some care systems actually and directly and measurably make a lot more money when the blood sugar isn’t managed and when people go blind and those same care sites make no money when people keep their vision and keep their sight and don’t need their care.
Every business in every industry does what it is paid to do. Most businesses are very clear about what that is and most business try aspire and try to do more of what it is paid to do. The care sites for the amputations in this country know that fee-for-service Medicare simply will pay them with no questions when amputations happen.
Medicare Advantage Costs Today’s Members Almost $2000 Less Per Member Per Year
Medicare Advantage care teams create better lives and much less cost and expense by getting that right. They are winning at multiple levels be getting it right and are much less costly for each member.
Medicare Advantage, as a package of costs and benefits, works so well today that the members spend, on average, $1900 a year less on care. That savings number achieved for each Medicare Advantage member was $1700 last year.
Care costs less and actually gets better when we create and fund the right cash flow for making care better and the members benefit financially and physically when that happens.
Economists should be clearly both understanding and explaining to us all that any care purchasing approach that buys care only by the piece is inherently flawed and limited because there’s actually no money in that piecework financial model or that piecework cash flow to improve care and because the actual painful functional reality is that the cash flow and profits for those care sites very often goes down significantly if care for their patients gets better and it actually does goes up when their care fails a patient.
That isn’t an ideological or political claim. It’s a biological and functional claim and a functionally mathematical claim and it’s obviously true in the real world.
If you cut the number of people who are admitted to hospitals for congestive heart failure crisis, then you save money for the payer, but and every fee-for-service hospital that doesn’t get the congestive heart failure admission loses $40,000 in revenue for each of those patients.
They hate losing patients. But that impact is very real and it’s actual money they don’t get when care improves.
Interestingly — and tellingly — that number also disappears from the $4 trillion we spend on care because that expense does not happen in the $4 trillion flow of cash when that care is not needed.
We have healthier patients, and a significant reduction in actual total money spent on care also happens directly each time we reengineer care to make some element of care unnecessary and then actually have it disappear from the flow of cash.
We Now Spend $4 Trillion on Health Care — Buying it by the Piece
Our goal should be to tee up the highly positive outcomes that can relatively easily actually result when caregivers with the right cash flow use that cash flow in intelligent ways to improve care and to make it more affordable and then take out of the expense levels care we don’t need to help bring that $4 trillion to a lower level.
We should also be negotiating prices on pieces of care — but do that in the context of a capitation cash flow where the internal payer is designing the processes of care and not just picking up the costs of pieces of care with no process in place as a guide.
Medicare Advantage does exactly that — and it’s a very workable model.
We have done process engineering in every other industry, and we have only tapped lightly into that continuous improvement space for care because we are almost always inept purchasers of care rather than being competent and intentional care buyers across most settings and because we have very poor standards on our quality components and we far too often reward damaging outcomes rather than rewarding better outcomes and better care.
We need Medicare Advantage to use the skill set they have by being care systems and the incentive they have by being capitated, and we need them to channel that set of incentives and resources into other markets to be a better buyer of care for additional payers.
Our goal should be to spend our cash to buy the care outcomes we want and that will only happen in the care settings where we function as a buyer and not a payer and then we up a cash flow that has the care teams in a setting making more money collectively by doing care right rather than by doing it wrong.
The very best opportunity we have to do that is to build on the capitated performance model that exists for Medicare Advantage plans today.
Critics Distort the Truth and Blame Upcoding for the Cost Difference and Plan Successes
People who are Medicare Advantage critics and opponents often say that the reason the Medicare Advantage plans have lower capitation levels than fee-for-service Medicare in all of the counties is because the plans have managed to refine and protect an “Upcoding” process for the risk pool calculations that distorts and inflates cash flow levels for plans.
Some critics still say that Upcoding by plans create roughly a 9 percent distortion level on the data and they say that we can’t believe that any of the obvious savings that create very visible surpluses in all of the counties are actually savings because those upcoded numbers drive the payments.
The MedPac staff wrote a dozen pages of their current annual report on Medicare Advantage listing historical largely anecdotal examples over two decades of various Medicare Advantage plans who they say managed to file reports about their patient risk levels that the MedPac critics labeled intentional Coding distortion and even Coding fraud relevant to their capitation levels and cash flow.
They warned the country again this year that distortion from Coding enhancement would still be at 9 percent for this year.
Their argument about the plans using those upcoded numbers to increase their profits always skipped the point that none of the plans actually needed any upcoding under the old system because the plans already averaged about 20 percent discounted costs from the available capitation numbers and because the Medicare Advantage plans also had profit limits written into both the contracts and the Affordable Care Act.
They do, however, want people to oppose plans for some reason, and so the current MedPac report still has anecdotes from prior years about some plans doing some things in those years to make their risk pool look less healthy. The anecdotes on those incidents that the people writing that annual report continue to repeat in their annual discussions of the program each year seem to be included in the report by members of that communications team who want to do brand image damage at some level to health plans and who want to skew the perceptions of the Commissioners against the actual plans without having any current data or evidence.
CMS Eliminated the Coding Process — Upcoding is Impossible
The truth today is — CMS completely eliminated that entire coding process two years ago and plans for the last two years of filings had no way to upcode anything.
They no longer code.
What made this year’s inclusion of that upcoding threat by plans in the MedPac report particularly wrong was that CMS very clearly actually changed the risk data flow into the process and they made upcoding by the plans completely and totally and functionally impossible.
They renewed that ban for 2023.
That ban on codes has to create some frustration in some academic settings, because very intelligent people in a wide range of academic programs in a wide range of settings have developed significant expertise into the old coding system over the past several years — and those thinking teams having been putting together research to see how much upcoding was going on then and now. Those academic teams were trying to estimate the impact of the upcoding on the cash flow. Their work and even field of expertise are now entirely obsolete relative to that entire area of health care economics because they have nothing to study.
Upcoding is now absolutely impossible.
Upcoding can’t happen.
Upcoding has no opportunity or vehicle to exist in today’s Medicare Advantage program.
What CMS does now to gain diagnostic information is both extremely accurate and highly usable as a source of data about Medicare Advantage payments. CMS now gets an encounter report on each encounter with each Medicare Advantage patient and they use that as the data base for those members.
Getting encounter information on each patient is a highly accurate and extremely timely process. The encounter report explains what happened for each patient, and it contains a diagnosis from that care site for that patient at this moment in time. CMS knows more about the patients and the care sites than it has ever known — and there are extremely competent experts using that data to understand and document key elements of data for those patients and their care levels.
The Medicare Advantage Bids are Lower than Average Medicare Costs Every Year
The Medicare Advantage capitation system is an extremely functional, very useful, and highly relevant system based and anchored entirely on the data base that exists for fee-for-service Medicare in every county in the country. We use actual current Medicare Data to set the cost levels and goals and our goal is to have Medicare Advantage costs below fee-for-service Medicare costs everywhere.
We start with actual Medicare current costs by county for the bids every year.
Fee-for-service Medicare has their claims payment data base for each county in the country and that set of paid claims is exactly what it costs us to pay for Medicare Beneficiary care under traditional Medicare now. That is highly accurate and very current data and it shows us exactly how much it costs to deliver traditional fee-for-service Medicare services in every county today.
If one of our goals for the Medicare Trust Fund and for the future costs of Medicare everywhere is to have those costs actually go down for the country in the future, then we can only do that if we know exactly what those costs are now in order to both set those goals and to put tools in place to make that reduction happen.
The original proposal for the first versions of Medicare Advantage back in the 1980s was to buy all of the Medicare benefits for anyone who wanted to enroll and to do it for 95 percent of the average costs of Medicare in every setting. That strategy required us to figure out the current costs of Medicare everywhere and to use that as the starting point of the process and that was a very good idea because it’s what we actually pay for that care.
We now know what the current costs are for traditional Medicare in every county. We give the plans that average cost number every year and we ask the plans to each give CMS a capitation bid that will buy that set of benefits for each plan for each county.
That bid from each plan is the cash flow that will happen for each plan — and no plan can ever go back to Medicare for more money even if the costs of care and or the benefits exceed that capitation amount. Medicare Trust Fund is guaranteed to achieve whatever savings are built into each bid because capitation is a one-way street on expenses and once it’s paid, the cost for each patient is done.
The plans use that flow of cash, and design their own additional benefits and make them available to the members as an enticement to join the plans and to stay with the plans. Standard fee-for-service Medicare and the total out of pocket costs of the standard member is now averaging about $5000 per year per patient.
Medicare Advantage members have both richer benefits and lower costs. They tend to have significantly better team care and far better benefits. That is particularly useful and attractive to the lowest-income members.
Low-Income Enrollees Love Medicare Advantage
Low-income enrollees love Medicare Advantage.
More than two out of three of the lowest-income Medicare beneficiaries from all groups have now joined plans More than 50 percent of the African American Members and more than 60 percent of the Hispanic members are now in plans as well.
The average net worth of all Medicare Beneficiaries is over $100,000 and the average net worth of the two thirds of Hispanic members who are now in plans is under $14,000. That net worth number is relevant to the differences in the benefits for the members. Traditional Medicare is very narrow in its benefit choices. Medicare Advantage plans use their surpluses to increase the benefits for their members. The Medicare Advantage plans overwhelmingly have vision benefits, dental benefits, and hearing benefits, and the patients who have only $10,000 in actual net worth tend to choose the plans that allow them to see and hear and even chew when that is possible to do. The plans all fund the additional benefits from the surpluses that they earn by having fewer crisis interventions, fewer amputations, and fewer people going blind.
There are many Medicare Advantage critics who oppose those additional benefits created by the surpluses and some say they oppose them because they are a new expense for the country and they somehow put additional pressure on the Medicare Trust Fund cash flow and they create expensive future expectations for Medicare members simply by being offered.
There is no new obligation because they are funded entirely by the average cost of Medicare in every county and this is a better use of the Medicare dollar and not new money.
The truth for anyone who understands the delivery of care is that traditional fee-for-service Medicare is inept, ineffective, incompetent, and far too expensive as a payer because it has way too many people who are losing vision and limbs at great expense to Medicare, and the very best use of the Medicare Trust fund from a pure economic perspective is to use the Medicare Advantage plans to buy far better care for significantly less money and to provide vision benefits rather than having people go blind.
The people who continue to voice that concern about the additional Medicare Advantage benefits should look at the source and creation of the funds and to should recognize and celebrate that people who can see better and people who hear better are less likely to be depressed and anxious in low-income settings.
The most amazing shortcoming and an almost ethical and humanitarian deficiency and inadequacy of the Medicare Advantage critics who continue to oppose the program at so many levels is actually the fact that nothing else in the country does so much direct support for people damaged by the Social Determinants of Health in real time and at large scale as the Medicare Advantage Special Needs Plans who deal with people who have dual eligibility today for both Medicare and Medicaid.
People with the Highest Care Needs and Lowest Income Join the Special Needs Plans
Social Determents of Health has become a new topic and a new awareness for us as a country, and it is a very good thing that we have a growing concern at multiple levels as a country about how many social determinants of health levels of damage have happened to people in this country reaching back decades in time.
We have seen prejudicial care, discriminatory and inadequate care, and we have seen extremely difficult differences in access to care — and we know that many of the people who have been most damaged by those shortcomings and those deficiencies are older Americans who have dual eligibility today for both Medicaid and Medicare.
The Special Needs Plans for Medicare Advantage are a very special program and the Medicare Advantage critics with their extremely rigid opposition to the program act today as though it does now exist. The same people who actually say that “Upcoding risk levels” is the business model of Medicare Advantage plans are trying to hide 4 million extremely relevant low-income and high medical-need people because the special needs plans doesn’t fit the paradigm they are trying to get us all to use.
One Medicare Advantage major critic in a policy think tank setting said in an actual policy and research piece last year that the dual eligibility enrollment should not be included in the discussion of how diverse the enrollment in Medicare Advantage actually is because they are so different that they should not count and their numbers should be invisible in the discussion of this entire process and of the diversity of the enrollment.
That think tank actually defined them out of the context of diversity as being outliers. That’s a very strange way of defining diversity.
The team at MedPac who are so opposed to Medicare Advantage wrote a report on the people with dual eligibility for Medicaid and Medicare and they compared their data to Medicare members who aren’t dual eligible and MedPac actually managed to write that report about dual eligibles without mentioning that Medicare Advantage even exists for those people and has clearly and visibly done extensive care enhancements targeted explicitly at those patients and has 4 million enrollees.
That stunning omission of care performance by MedPac belongs in a False Positioning Fake News Hall of Fame because the data is absolutely clear that the people with Medicare Advantage from that group are half as likely to go blind and that’s because Medicare Advantage is managing the blood sugar of their patients to change that outcome and that has happened because of the care teams that so visibly exist even in the advertising for the special-needs plans.
That far better and patient focused care program is not invisible to those 4 million people. Those 4 million people basically know from their daily interactions with the care system how many blessings they are getting from that care and they have better lives at many levels
As special needs plan members with significant multiple health care needs, each of those members have extensive in-home benefits and services, team care, and many are now getting team care and patient focused care for the first time in their lives and love it.
That information should be a foundational part of what we all know about Medicare Advantage and the news media should be reporting every year on the improvements being made each year in their care and in the program for Medicare Advantage and only Modern Health care is writing about them in the health-care press.
The truth is that many of those dual eligible members are getting the best care of their lives and the government is now doing all of that care for significantly less money than they spend on those same patients when they are not in the plans.
The dual needs people who are getting care as a package have much better care for significantly less money because it costs less to do it right even for our highest need patients.
It was particularly good timing for those low-income and high-need people to be enrolled in plans before Covid hit. Every one of those high need people had their health plan on their side immediately with real functionality and context for the Covid process. Fee-for-service Medicare had no programs or support or infrastructure for those patients — and everyone enrolled in a plan had the comfort of knowing they were in a Medicare Advantage Plan and had support in place.
The Covid death rate for that set of patients in their fee-for-service settings was 22 percent. The Covid death rate in their Special Needs Plans was 15 percent. That is a major difference and MedPac also refused to cover, discuss or describe that entire array of those performance differences between the two approaches for Covid patients because that information about how much better the plans did at multiple levels for the Covid patients didn’t fit the message that some people at MedPac are so strangely but deeply committed to perpetuating about the value of the program.
One of the most useful points to make is actually the data that has emerged for CMS in having the actual information from the encounter reports about each of the Medicare Advantage patients.
CMS understands the program.
The people who run CMS are doing amazingly good and grounded work with the Special Needs plans and with the Dual Eligibles. They know the program and they clearly understand its massive value, and they are steering it in good directions in continuously improving ways. The absolute gap in competence from the MedPac reports have no parallel stream with the actual people at CMS and they are enhancing each of their reporting competencies in very intentional ways.
They have not gone to the Media with their insights about those patients, but their new 2023 rule kit for Medicare Advantage is extremely well done and on track. They took the actual extremely accurate data they now have about all of the Medicare Advantage members from the encounter reporting system and they used the actual data about the actual members to determine that the actual enrollment says that they should increase capitation levels for the plans by 8 percent for next year.
That information stunned all of the Medicare Advantage critics who said that their coding concerns had pointed them in exactly the opposite direction on the actual risk status of the member. That conclusion means that their more accurate data showed that the plans are being slightly underpaid based on the value and care level and based on the actual health status of the members.
That higher than expected percent capitation increase number is creating a fascinating market dynamic for the country, because the plans have all been creating surpluses already with their old bids at the lower capitation levels and there’s no way for them to use the additional money.
So the plans will now need to decide and announce what their bids will be for 2023. That should be a significant media story when it happens because it will affect so many millions of people and will give us a sense of future product designs for the plans.
Those discount decisions from the plans are due relatively soon. They could be the biggest discounts ever since capitation began. That’s good for Medicare because every penny of discount in those bids is direct dollar-for-dollar savings for the Medicare Trust Fund.
Medicare will have a longer life if the 2023 plan discounts are high and if they create real financial savings for Medicare for those members. The plan discounts this year might be very high — because Medicare fee-for-service care continues to be so bad — and the discounts are lower costs for the trust fund.
We need everyone to know that it’s good for people to not be in many of those flawed care settings and that their lives will be better with better care. We can measure some of that progress for patients. We know that last year, 17.1 percent of the diabetes patients in fee-for-service Medicare settings experienced diabetes related cellulitis, ulcerations, osteomyelitis, gangrene or amputation and we now know that the plans have done the right things for those patients and reduced that risk to 8.2 percent of the diabetic patients, that will cost significantly less money.
The reality and the irony of that situation is that the capitation being offered with an 8 percent is structurally and legitimately based on the 17.1 percent of the fee-for-service Medicare patients being at those higher levels of expense and risk but it is more money than the plans can use because the plans already have maximized their ability to keep the profits created by their current discounts on capitation.
The news media and health economists should be watching that like a hawk because it will affect health care costs and benefits for millions of people, but most don’t have a clue that the situation actually exists or that the plans now need to make those decision.
The most interesting sets of financial decisions being made in America now will be based on that context and they will set up a major portion the future cash flow for the country through purchasing channels, and the amounts of money are extremely high for that process.
That is proven absolutely, completely, and currently by looking at the actual bidding process being used for 2023 by CMS for Medicare Advantage. It’s a very visible process if you know where to look. These powerful and highly directional specifications clearly are structuring the future delivery of care for all of the capitated people.
They also prove that the upcoding concerns of the past no longer exist, because it is clear in the 2023 requirements that the old coding system is dead and it has been replaced again by only getting that information from the actual encounters that happen for each Medicare Advantage member.
That change is clearly stated early in the bidding document.
So we know that the issue of Upcoding now is absolutely fake news and we know that the issue from the Medicare Advantage critics and opponents of health plans somehow skewing cash flow for the country by sending nurses into homes to “harvest diagnosis” and by hiring too many consultants who have the ability and assignment of changing risk pools is voodoo economics, urban legend and impossible to achieve.
We are definitely in interesting times. We should change the politics of health care future funding and current costs to focus on the real numbers created by both purchasing approaches and then we should become better purchasers of care rather than inept payers for care by encouraging Medicare Advantage enrollment.
The Five-Star Program Changes the Culture of Care in Some Settings Who Now Take Great Pride in Achieving Four and Five Stars
The very best Medicare Advantage plans do wonderful and spectacular work. We are seeing the number of plans who earn four or five stars on the Medicare Advantage five-star plan going up from a couple of percent to more than 80 percent of members enrolled — and that growth in the number of plans achieving those performance levels is solid evidence for the fact that the entire package is working.
The Medicare Advantage Five-Star Plan has had a major and unexpected impact on the culture of American health care that we need to understand, appreciate, and build on.
We have not had a culture of continuous improvement or of high quality in health care in America. Most of our care sites believe by nature they are excellent or even perfect and very large number of sites believe that they deliver the best care around.
The number of Heart Surgeons who will say that they are not the best available heart surgeon is a very small list.
The self-confidence of those care sites has not been universally validated by data far too many times. We have not made measurement of quality in order to validate and to continuously improve it a process that happens in the vast majority of care sites, and the Medicare Advantage five-star plans has been a needed and welcome outlier in that agenda.
As a country, we have not measured care well in many areas and in many settings. It is very difficult to introduce care improvement agendas into most care settings. Leaders in those settings sometimes try, but the number of people who run and direct Medical groups, care settings, and health plans who can, on their own personal credibility go the folks at their care site and simply say — “I, as leader here, think we can do much better on diabetes care,” is surprisingly low.
Leaders who decide to make those kind of statements and who try to lead in those directions in most care sites on their own conviction and credibility are highly likely to be rejected, unheard, opposed, or even deposed if they make the care improvement suggestion with too much vigor.
Caregivers tend to have a sense that their care is darn good, and don’t want even their own leaders to measure or judge them in many areas of their care.
That has left a huge gap in care.
Most hospitals did not even keep any kind of record of mortality rates that might be linked to a caregiver because the caregivers all reject those kinds of measurement and a high percentage believe that there’s no legitimate way of measuring any of those issues and that care improvement isn’t really needed.
Malpractice suits actually are the only safety net for patients in too many areas because nothing else exists or can be done for those care settings.
Medicare Advantage has helped with that issue and those barriers hugely — in ways that almost no one who isn’t running a care system might understand.
Medicare Advantage created the Five-Star Plan and got very specific about some areas where everyone should be delivering some levels of care.
Medicare Advantage cracked that barrier to measuring care in those settings by creating that plan. They put in place a few real goals — like measuring the blood sugar of diabetics — and then they actually paid the plans up to 5 percent more money if they achieved five-star ratings with those goals. The money made it real enough and credible enough so that that the leaders who ran each of those care settings could say, this is win-win. We win. The patients win. Let’s earn five stars for our care and all win.
Skillful leaders in multiple settings have loved having that resource to introduce that set of behaviors into their organizations. They have used that template to help set up a culture of achievement in those settings — and the plans who earn three stars or four stars or five stars celebrate those wins with culture affirming communication and events.
It’s a game changer. It is now a big thing in many care settings and many communities to be a five-star plan. That’s wonderful for the quality of care in America because it gives us a paradigm of expecting and rewarding high performance for both service and quality and being ‘five-star’ has its own level of pride and accomplishment as part of the process.
The people at MedPac who have criticized that five-star program so often and so interestingly vaguely clearly have absolutely no awareness of most of the things that it does, and the MedPac people clearly have no awareness of and process improvement approaches, cultures or context, because they never mention any of those issues in their mildly disparaging comments. The reality is that there might not be a quality program for any government in the world that does as much good as the Medicare Five-Star program does for us and the MedPac people have suggested it be replaced by something that is not so plan specific.
It’s a new cultural expectation for many care sites to have top rated care as a process and a goal, and that’s actually another good reason to support the Medicare Advantage program.
That program very directly strengthens the hands of CMS as a buyer. The CMS crew looks hard at the current five-star goals and does very enlightened things to use them well. CMS should get five stars for how well they have recently done that.
The beauty and the genius of being a buyer rather than a payer is that you can insist on performance as a buyer and you can steer entire markets to those better care opportunities using those levers.
We need the policy world to look hard at what CMS is putting in place for the Dual Eligibles for this year and next, and we should encourage and celebrate what they are doing because that set of patients has been most damaged in the past by care inequities and care inadequacies and they are now getting individually focused team care and much better care outcomes.
MedPac continues to have hard core critics who are clearly committed to putting Medicare Advantage in the worst light and they continue to not tell the real story to Congress and the American public. They actually wrote in their annual report again that a major concern for the country this year should be upcoding — and they predicted it would happen again even after they all knew that the coding system actually completely disappeared.
They also wrote a report on the dual eligibles — showing extensive data that makes clear the differences in care patterns for the dual eligible and the single eligible people — and they completely left out of their report the obvious point and fact that 4 million of those people were enrolled in Medicare Advantage and had much better care.
Congress should increase their performance expectations for MedPac and should say that their job should be to get the optimal use out of the Medicare dollar rather than trying to reduce the number of dollars being spent on Medicare. Getting optimal use reduces the costs of Medicare and the beneficiaries should be entitled to having Medicare purchase care well.
If we continue to support Medicare Advantage approaches on care delivery, that will have a broader impact on all of care because there will be spillover impact on the vast majority of care delivered in America just because it is so difficult for care sites actually functioning in care delivery to set up two or more approaches to care.
Best practices can come into being through that back door for many patient. Medicaid plans across the country who are capitated have those same financial incentives and use many of the same tools — and that puts us on a path to have the tool kit in some of those areas become the new normal for America.
If the new normal for American health care is having half as many kids going through asthma crisis and half as many seniors going through congestive heart failure crisis, that’s a good new normal to have.
We Need Best Practices and Continuous Improvement to Be the New Normal for American Health Care
We should make the decision as a country that it is bad and inferior and damaging care when we have 30 percent more hospital admissions for some discharges and 40 percent more hospital admissions for other diseases, and, in the real world for real patients, those higher admissions are an obvious and unacceptable failure of care for many of those patients. Too many people are damaged by bad care — and we should stop accepting those failures as being just what happens for fee-for-service Medicare Patients.
Minimally, we need Medicare to provide information to all members that those difference in care exist.
Traditional Medicare has some sites that include Accountable Care Organization care teams who use some of the same approaches that Medicare Advantage plans use and get some of the same results because we all have the same biology and those same issues exist everywhere.
We should try to help people who don’t get the full benefit of Medicare Advantage to go down those Accountable Care Organization paths. We should support those organizations and we should also do what we can to enable them to become Medicare Advantage plans with the lowest barriers and significant support where needed.
As a nation, we should be on the cusp of a golden age for care. The new tool kit should give us better diagnoses, better care plans, better team care, better follow up and better care connectivity. Some of the new science linked tools can predict with a very high level of accuracy who will be having a heart crisis within the year — and we need those tools to be available to everyone.
Some of the best Mayo like tertiary care sites in history exist now and those sites and care teams are creating some exceptional care at this point in time and putting in place some spectacular science about care — and we need Medicare Advantage plans that will take full advantage of those tools as part of the nature of who they are and because they will be more competitive and less expensive with those components built in.
We are seeing complete hospitals set up in homes that are lower cost, high quality and a much better option at several levels for some patients today.
Medicare Advantage plans will use them because their capitation model favors better care at lower cost. That isn’t entirely speculation. One of the biggest new systems of in-home hospitals was co invented by the Mayo Clinic and by one of the original Medicare Advantage plans.
We need Medicare Advantage plans to use those tools as well.
We need the critics of Medicare Advantage to stop saying things that they know are not true when they say them. Being a critic of the program is fine and good and even performance enhancing — but saying the business model of plans is to harvest risk codes is getting old and distorts the discussing in damaging ways that we need to get past.
We need to reengineer care — and we need a cashflow template to make that happen and to use that better care when it happens.
One Medicare Advantage linked hospital system looked at the death rate from Sepsis and decided to re-engineer care to get down. More people die of sepsis than any other disease in American hospitals.
That system had a sepsis death rate of over 20 percent when they started the process. So they engineered every part of the system. They did early diagnosis, early prescribing and focused interactions and they dropped the death rate to 10 percent and then to 5 percent, and then to about 3 percent.
There is a golden half hour in Sepsis care, and the care team modified processes to make that care happen. They made filling the sepsis prescriptions as a top priority for the pharmacy a point in the process to cut 30 minutes from the process and they then decided to put the sepsis drugs prepackaged on each hospital floor to cut 20 more minutes from that process.
For most hospitals, sepsis patients are very profitable. For a Medicare Advantage hospital, the sepsis patients were pure and total expense — and the expenses were considerably lower in those sites when the new length of stay dropped from weeks to days and when almost everyone survived.
Everyone in America deserves that level of care in the hospital. That’s the number-one cause of death in America and great care is more likely to happen when the care setting is capitated in some way.
The number of hospitals with that level of enhanced sepsis care is very low. The number of hospitals who are doing amputations because the diabetic care for patients with foot ulcers is failing is far too high.
We need to get that level of systematic, process-oriented care in place across our sites of care — and we will be more likely to succeed if we use Medicare Advantage plans to set up the template for all care across multiple care sites.
We can change the amputations — and that is most likely to happen where patients have care teams.
We are spending $4 trillion on care today. Medicare Advantage is almost the only component of the health care funding and purchasing agenda that has a chance of turning a higher percent of that $4 trillion into better and less expensive care. We need to understand what it does and then create expectations for the rest of care that involved systems supported continuously improving care for as many people as we can.
That 15 percent tax, collected just like the Social Security tax we use now for our Social Security funding would give us a guaranteed and more than adequate payment fund to buy universal coverage for all employed people that would actually give us enough money to pay a Medicare Advantage capitation for every employed person in the country. That tax would not be an increased cost. It would actually be a reduction in the amount most employers pay now to buy their current health insurance coverage and would actually be less than the employers who provide coverage spend now for care.
The 15 percent could be split with the employees in various ways. Germany, Switzerland, and The Netherlands all use the 15 percent and split it 50-50 with the employer and employee and the employees all buy capitated Medicare Advantage like health plans with the capitation.
That 15 percent tax would also let the low-income pay-rolled companies in our country who don’t provide coverage now afford to pay for their coverage because the current cost runs closer to 25 percent of payroll for employers with low paid employees to buy care in the current insurance market and the tax would be a major cost break that would make care affordable for them as well.
That’s not the key point of this piece, however.
The point is to have people understand how extremely well done the Medicare Advantage plans do now in providing coverage to the Medicare people they cover and to suggest that we should extend that level of protection to everyone on Medicare do what we need to do to stop having so many people having amputations and going blind from bad care.
And we should protect Medicare Advantage from the die-hard critics who are impervious to data, facts, accomplishments, performance levels, cost savings and care outcomes and who seem to just want to kill the plans because they have a deep-seated hatred for anything that functions in that capacity and that has that structure.
The people who hate plans ignore how badly the traditional fee-for-service Medicare care delivery works and how many people it damages, and they just want the plans to die.
The good and encouraging news is that no one in any position of legitimacy in the government believes what they are saying, and the people who run CMS are providing strong support to the quality agendas and to the Special Needs Programs and to the retiree plans and the people who actually run Medicare are making each of those programs better with their specifications each year.
The people who run CMS understand the Affordable Care Act tool kit and they are building on it with great competence.
They have a strong sense of mission, vision, and destiny for the dual elegible special needs plan people and for all of the other high need people, and they are also building a wide range of extremely credible Accountable Care Organizations (ACOs) that all make care better and that also spend less money doing it.
At this point, the only people who can’t see that care costs less when you engineer the processes are the health care economists and health policy people who have not learned anything about care improvement and who still feel at some point of principle that it’s better for Medicare to buy care entirely by the Piece and to have it function entirely on its own doing its own flawed and damaging sets of things.
It would be a good thing if this piece helped some of those people who have been critics enhance and embrace that paradigm and direction.
We should be moving into great care. Let’s support that agenda and make it happen.